For Your Healthcare Provider
Have your patient scan this QR code with their smartphone camera to instantly access this educational guide on their device.
A guide for patients with low iron stores and normal hemoglobin
Access the Resources
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
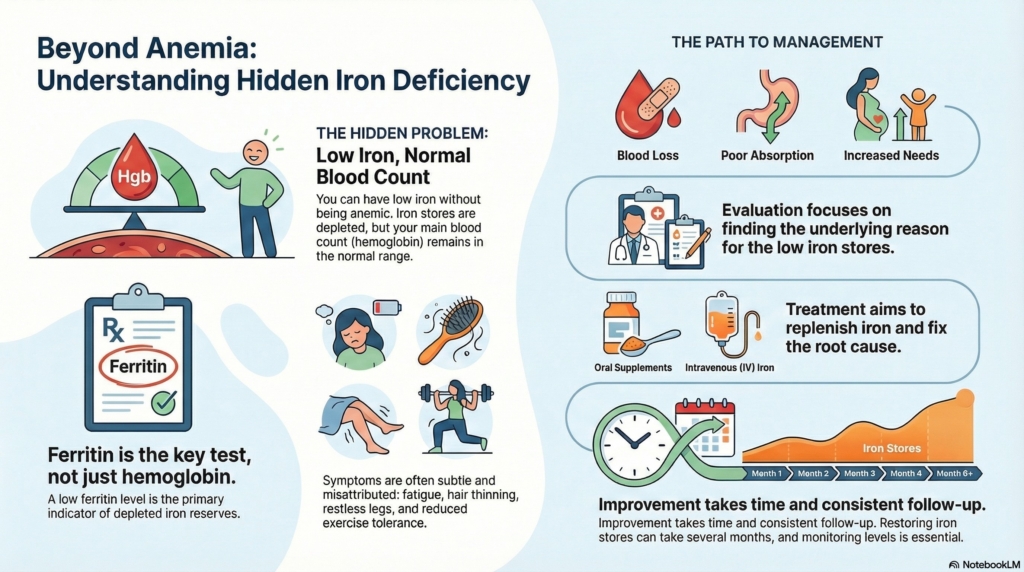
Iron deficiency without anemia means your iron stores are low, even though your hemoglobin is still normal.
This is common, often missed, and very treatable. Some people have symptoms before anemia develops, while others feel completely well.
The goal is to understand why iron is low, whether it explains symptoms, and how to rebuild iron stores safely.
First things first
Iron deficiency without anemia means that the body’s iron stores are low, but the hemoglobin level, the blood test used to diagnose anemia, remains within the normal range.
This finding is common and often missed because many people assume iron problems only matter when anemia is present. In reality, iron plays roles beyond making red blood cells, including muscle function, brain chemistry, and energy metabolism.
Doctors evaluate this condition by looking at iron studies, especially ferritin, rather than hemoglobin alone. The goal is to understand why iron stores are low, whether symptoms are related, and whether treatment is appropriate.
What it is
Iron deficiency without anemia is sometimes an early or “pre-anemia” stage of iron deficiency. It means the body does not have enough stored iron to meet its needs, even though hemoglobin remains normal.
Ferritin is the most useful test for assessing iron stores. A low ferritin level indicates depleted iron reserves, even if hemoglobin and other red blood cell indices remain normal.
In some people, this represents an early stage of iron depletion. In others, iron stores remain low for longer periods while the body keeps hemoglobin in the normal range, sometimes at the expense of other iron-dependent processes.
Why it happens (causes)
Iron deficiency without anemia develops when iron losses or iron needs exceed intake or absorption.
For many people, it helps to think of causes in broad terms: iron may be lost over time, not enough iron may be coming in through the diet, the body may have trouble absorbing iron from the gut, or iron needs may be higher than usual. These factors often overlap, and more than one may be present at the same time.
Common contributors include:
- ongoing blood loss, most often from menstrual bleeding and sometimes from the gastrointestinal tract
- reduced dietary iron intake, particularly in people who avoid meat
- impaired absorption from the gut, including conditions such as celiac disease, prior bariatric surgery, chronic use of acid-suppressing medications, or certain infections
- increased iron needs during growth, pregnancy, endurance exercise, or with frequent blood donation
Inflammation can also complicate interpretation, because ferritin may appear normal or mildly elevated even when the body does not have enough usable iron.
Does it cause symptoms?
Yes, it can.
Some people feel entirely well, while others experience symptoms that improve once iron stores are replenished. Symptoms may develop gradually and are often attributed to stress, sleep issues, or aging.
Common symptoms include fatigue, reduced exercise tolerance, difficulty concentrating, restless legs, hair thinning, brittle nails, and a sense of low stamina that feels out of proportion to daily activity.
These symptoms can overlap with many other conditions, which is why doctors look at the whole picture. In some cases, improvement after iron repletion helps confirm that low iron was contributing.
Is it dangerous?
For most people, iron deficiency without anemia is not dangerous in the short term.
However, persistent iron deficiency can progress to anemia, and long-standing low iron stores may worsen symptoms, reduce quality of life, and complicate other medical conditions.
In some settings, iron deficiency signals an underlying problem, such as ongoing blood loss or malabsorption, which deserves evaluation even if anemia is not present. This is especially important in adults who do not menstruate.
How your doctor evaluates it
Evaluation begins with a careful review of symptoms, diet, medications, and medical history.
Blood tests usually include ferritin, iron, transferrin saturation, and sometimes inflammatory markers. Doctors interpret these values together rather than relying on a single number.
If iron deficiency is confirmed, the next step is identifying the cause. This may involve gynecologic evaluation, gastrointestinal testing, or assessment for dietary or absorption issues, depending on age, sex, and risk factors.
Doctors often look at:
- ferritin to assess iron stores
- transferrin saturation to understand iron availability
- trends over time rather than a single result
- possible sources of blood loss, such as menstrual or gastrointestinal bleeding
- factors that affect absorption, including gut conditions or medications
What is the treatment?
Treatment focuses on replenishing iron stores and addressing the underlying cause.
Many people are treated with oral iron supplements, often taken once daily or every other day, depending on the plan you and your doctor choose. This approach can improve absorption and reduce side effects.
In some situations, such as poor absorption, intolerance to oral iron, or a need for faster repletion, intravenous iron may be recommended even without anemia.
Not every symptom is caused by iron deficiency, so your doctor may also look for other explanations if symptoms do not improve.
Daily life and self-care
Dietary iron can help support recovery, but diet alone is often not enough to correct deficiency once stores are low.
Taking iron supplements as directed, avoiding unnecessary interruptions, and understanding that improvement may take weeks to months can reduce frustration. Many people begin to notice changes within a month or so, while full restoration of iron stores can take several months.
Managing contributing factors, such as heavy menstrual bleeding or gastrointestinal symptoms, is an important part of long-term care, not just iron replacement.
Helpful self-care strategies may include:
- taking iron exactly as prescribed, even if symptoms improve
- spacing iron away from foods or medications that reduce absorption (for example, calcium supplements or antacids), if your clinician recommends this
- being patient with gradual improvement in energy or stamina
- addressing contributing issues, such as heavy periods or digestive symptoms, with your care team
When should I contact my doctor?
You should contact your doctor if symptoms persist or worsen despite treatment, or if new symptoms develop.
Follow-up is also important if iron levels fail to improve, if iron deficiency returns after treatment, or if you experience side effects that make therapy difficult to continue.
Prompt communication helps ensure that the cause has been adequately evaluated and that treatment remains appropriate.
Reach out to your clinician if:
- fatigue or other symptoms do not improve after treatment
- iron levels remain low or drop again after therapy
- side effects make it hard to continue iron supplements
- new symptoms appear that concern you
What is the usual plan going forward?
Most clinicians monitor iron studies over time rather than relying on a single test.
Once iron stores normalize, treatment may be stopped or continued at a lower maintenance dose, depending on the cause. Some people require periodic supplementation if the underlying driver cannot be fully corrected.
The long-term plan is individualized and may evolve as life circumstances, medical conditions, or bleeding patterns change.
Making sense of it
Iron deficiency without anemia sits in a gray zone that does not fit neatly into “normal” or “anemic.”
Understanding that iron has roles beyond red blood cells helps explain why symptoms can occur even when hemoglobin is normal. Addressing iron deficiency early can prevent progression, relieve symptoms in some people, and reduce unnecessary worry about unexplained fatigue or low energy.
Key takeaways
- normal hemoglobin does not rule out iron deficiency, and symptoms can still occur
- ferritin reflects iron stores, and low levels matter even without anemia
- most cases are not dangerous, but persistent deficiency should be evaluated
- treatment is effective, and improvement often takes time
- follow-up matters, especially if iron deficiency returns or symptoms persist
If you’d like to go deeper:
Our guide to living with iron deficiency covers diet, supplements, recurrence, and day-to-day questions that often come up after diagnosis or treatment.
If treatment is needed, our overview of oral versus IV iron therapy explains how these options differ in speed, convenience, and side effects
For clinicians: Read our detailed guide on how to communicate about non-anemic iron deficiency to patients.