For Your Healthcare Provider
Have your patient scan this QR code with their smartphone camera to instantly access this educational guide on their device.

A guide for patients with immune thrombocytopenia
Access the Resources
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
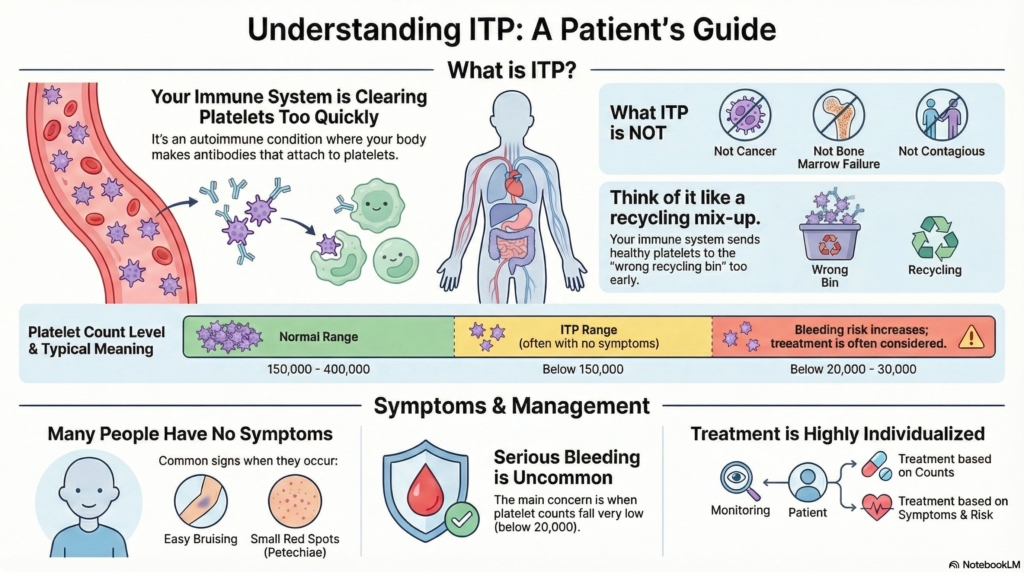
Immune thrombocytopenia (ITP) is a condition in which the immune system removes platelets too quickly, leading to a low platelet count.
ITP is not cancer, not bone marrow failure, and not contagious. Many adults with ITP feel well even with low platelet counts, and serious bleeding is uncommon in outpatient care. With monitoring and treatment when needed, most people do well and live full, active lives.
This guide is for typical outpatient ITP. If you have severe bleeding or rapid changes, contact your doctor right away.
First things first
ITP is a condition in which the platelet count is low because the immune system mistakenly targets platelets. A normal platelet count is usually between 150,000 and 400,000, but people with ITP may have numbers well below this range even while feeling completely well.
Most adults with ITP are otherwise healthy, and many cases are managed safely with monitoring alone.
What is immune thrombocytopenia?
Immune thrombocytopenia is an autoimmune condition in which your body makes antibodies that attach to platelets.
The spleen then removes these platelets from circulation, causing a lower-than-normal count.
Your bone marrow usually continues to make platelets normally, but they are cleared too quickly.
Why it happens (causes)
In many adults, the exact trigger is never known. Not knowing the trigger does not change how we monitor or treat ITP. Your body’s current pattern matters more than the original cause.
Possible contributors include:
- recent viral infections
- autoimmune conditions (like SLE)
- medications
- sometimes related to chronic infections such as hepatitis C or HIV
- occasionally following vaccination
For most patients, no single cause is ever identified.
Does it cause symptoms?
When symptoms occur, they may include:
- easy bruising
- small red spots on the skin (petechiae)
- bleeding with brushing teeth
- nosebleeds
- menstrual changes
However, many people have no symptoms even with very low counts, and severe bleeding is rare in outpatient adults.
Some people also report fatigue, which can happen with ITP even when bleeding is not present.
Is it dangerous?
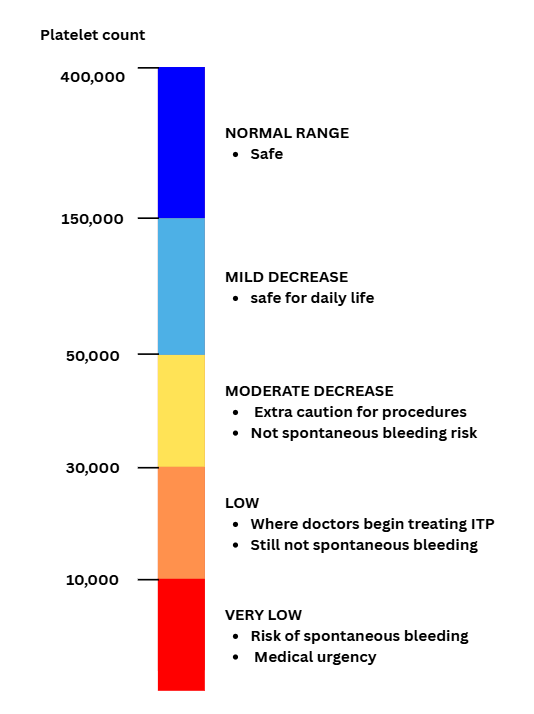
Bleeding risk increases mainly when platelet counts are very low. Many people with ITP have mild or moderate thrombocytopenia and do not have dangerous bleeding.
Most adults with ITP do not develop dangerous bleeding.
The main concern is when platelets fall below about 20–30,000, when spontaneous bleeding becomes more likely.
Even then, serious events remain uncommon.
Hospital care is usually needed only when platelet counts are extremely low or when there is active bleeding.
Some cases of ITP improve on their own within 6–12 months, while others become chronic and require ongoing monitoring.
How your doctor evaluates it
Your doctor will:
- review your history and medications
- perform a physical exam
- check blood counts (CBC)
- order targeted labs to rule out other causes
- consider bone marrow testing only if results do not fit the usual pattern or the diagnosis remains unclear
Most adults do not need a bone marrow biopsy.
How is it treated
Treatment depends on your platelet count, symptoms, and how quickly the numbers are changing.
Many people need only careful monitoring when counts are stable and bleeding symptoms are mild or absent.
Treatment is often considered when platelet counts fall below about 20–30,000, especially if there is bleeding or the number is dropping quickly.
When treatment is needed, options may include:
- short courses of steroids
- IVIG to raise the count quickly
- medications that help your body make more platelets (TPO agents)
- immune-directed therapies if the condition persists
- surgery to remove the spleen in rare situations when other treatments haven’t helped
Daily life and self-care
- avoid NSAIDs unless advised
- limit high-trauma activities when counts are very low
- routine dental care is fine, but may require planning
- monitor for new bruising or bleeding
- discuss pregnancy or surgery planning with your hematologist
Most routine daily activities are safe when platelets are above 50,000.
When should I contact my doctor?
Call your doctor if you notice:
- increased bruising
- nosebleeds
- heavier-than-usual periods
- small red or purple spots on the skin
- bleeding that is slow to stop
Seek urgent care for:
- vomiting blood
- black or tarry stools
- blood in urine
- severe headache
- difficulty breathing
- confusion
What is the usual plan going forward?
Most adults with ITP follow a pattern of:
- Regular CBC monitoring
- Watching symptoms
- Treating only when the platelet count or symptoms increase bleeding risk
Many people live full, active lives with ITP.
Making sense of it
ITP is like your immune system sending platelets to the wrong “recycling bin.”
Your body keeps making new platelets, but they are removed faster than usual.
ITP means your immune system is clearing platelets too quickly, lowering the count. Many people stay safe with monitoring, and treatment is used only when bleeding risk increases. Most adults with ITP do well long-term, even if the condition persists.
Key takeaways
- ITP means your immune system is clearing platelets too quickly, but it is not cancer
- many adults have few or no symptoms, even at low counts
- serious bleeding is uncommon in outpatient adults
- treatment is individualized, and sometimes no treatment is needed
- most people do well long-term, with safe, stable counts
For clinicians: Read our detailed guide on how to communicate about ITP to patients.