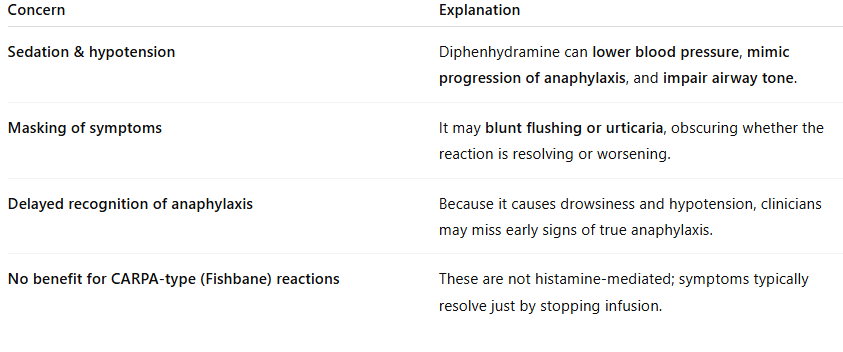
Because it can worsen the situation or mask the diagnosis.
- For many years, clinicians routinely gave diphenhydramine as premedication or treatment for IV iron reactions — borrowing habits from transfusion or contrast medicine.
- However, updated understanding of IV iron hypersensitivity (especially the CARPA mechanism) has changed this practice.
- Most acute IV iron reactions are complement activation–related pseudoallergies, not histamine-driven allergic reactions.
- Thus, antihistamines like diphenhydramine don’t address the underlying cause and may make clinical assessment more difficult.
When (and How) It May Be Used
Diphenhydramine is reasonable only in:
- Moderate allergic-type reactions with clear urticaria, itching, or angioedema after IV iron (especially if mild and non-progressive).
- Adjunctive therapy after epinephrine in anaphylaxis — never as first-line.
If used:
- Give 25–50 mg IV or PO after stabilization, not preemptively.
- Avoid routine premedication.
Bottom Line
Diphenhydramine is not contraindicated, but:
- It is no longer first-line for IV iron reactions.
- It should not be given preemptively or early in hypotensive reactions.
- It may be used selectively for urticaria after stabilization.