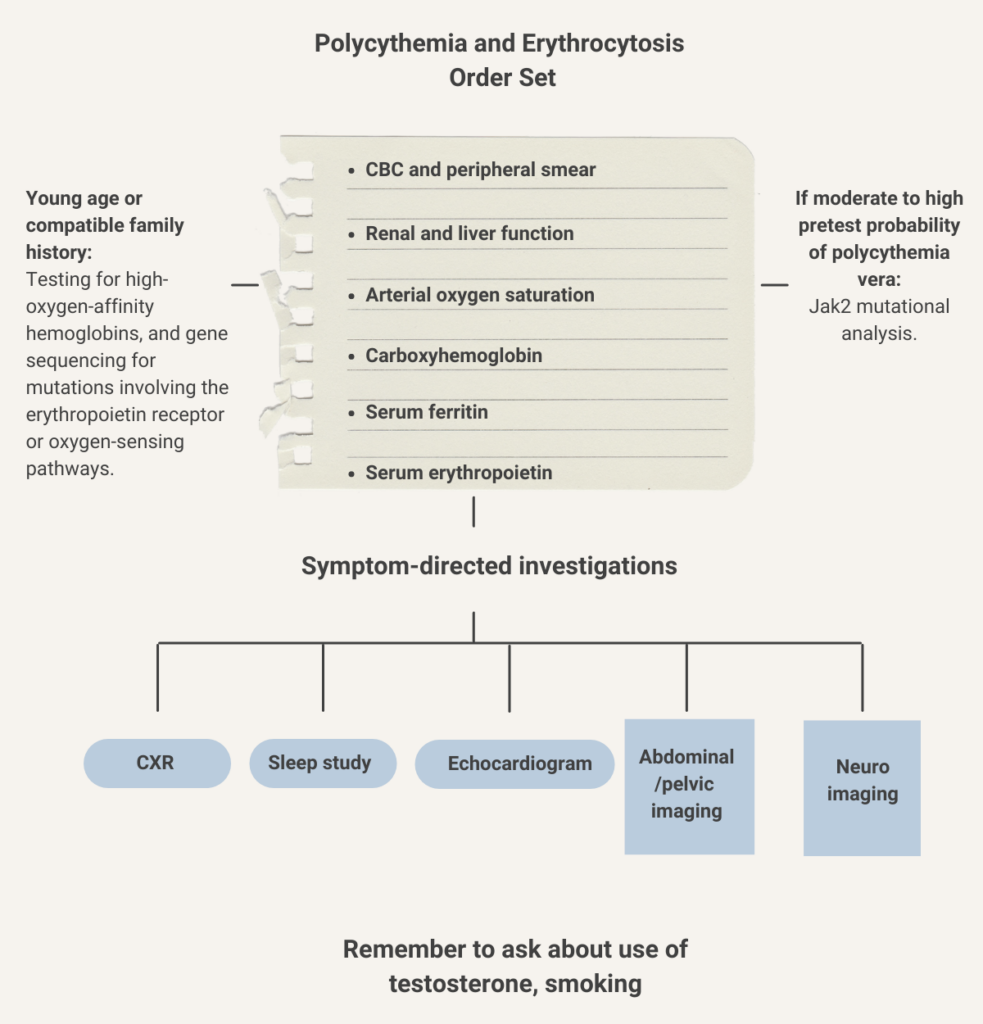
First-line testing:
- Complete blood count
- Peripheral blood smear
- Renal function
- Liver function
- Arterial oxygen saturation
- Carboxyhemoglobin
- Serum ferritin
- Serum erythropoietin:
- A low erythropoietin level (< 2.9 mU/mL) specific (92%) and moderately sensitive (64%) for the diagnosis of polycythemia vera.
- A high erythropoietin level (> 15.1 mU/mL) specific (98%) but had poor sensitivity (47%) for the diagnosis of secondary erythrocytosis.
- Jak2 mutational analysis (peripheral blood) – based on the pretest probability of polycythemia vera (PV):
- In the primary care setting, where the probability of PV is low, clinical evaluation for secondary causes of erythrocytosis paired with a high erythropoietin level can rule out PV in most patients.
- In hematology clinics, where the probability of PV is higher, erythropoietin level and JAK2 V617F mutation testing are done concurrently.
- Patients with a low or normal erythropoietin level and no JAK2 V617F mutation are further evaluated with JAK2 exon 12 mutation testing (on peripheral blood or marrow aspirate, based on local practice) and a bone marrow biopsy.
Second-line testing:
- When no diagnosis is made, selected patients with onset of erythrocytosis at a young age or compatible family history should undergo testing for high-oxygen-affinity hemoglobins, and gene sequencing for mutations involving the erythropoietin receptor or oxygen-sensing pathways.
- Investigations for secondary erythrocytosis should be symptom directed and may include:
- Chest radiography
- Overnight oximetry for suspected sleep apnea
- Pulmonary function tests for hypoxic lung disease
- Venous blood gas sampling (carboxyhemoglobin level)
- Echocardiography to rule out right to left cardiac shunting
- Abdominal–pelvic imaging can help exclude an erythropoietin-producing tumor or conditions associated with local renal hypoxia.
- Neuroimaging to rule out meningioma or cerebellar hemangioblastoma should be ordered for patients with unexplained neurologic symptoms as these tumors have been associated with autonomous erythropoietin production.
Learn more here.