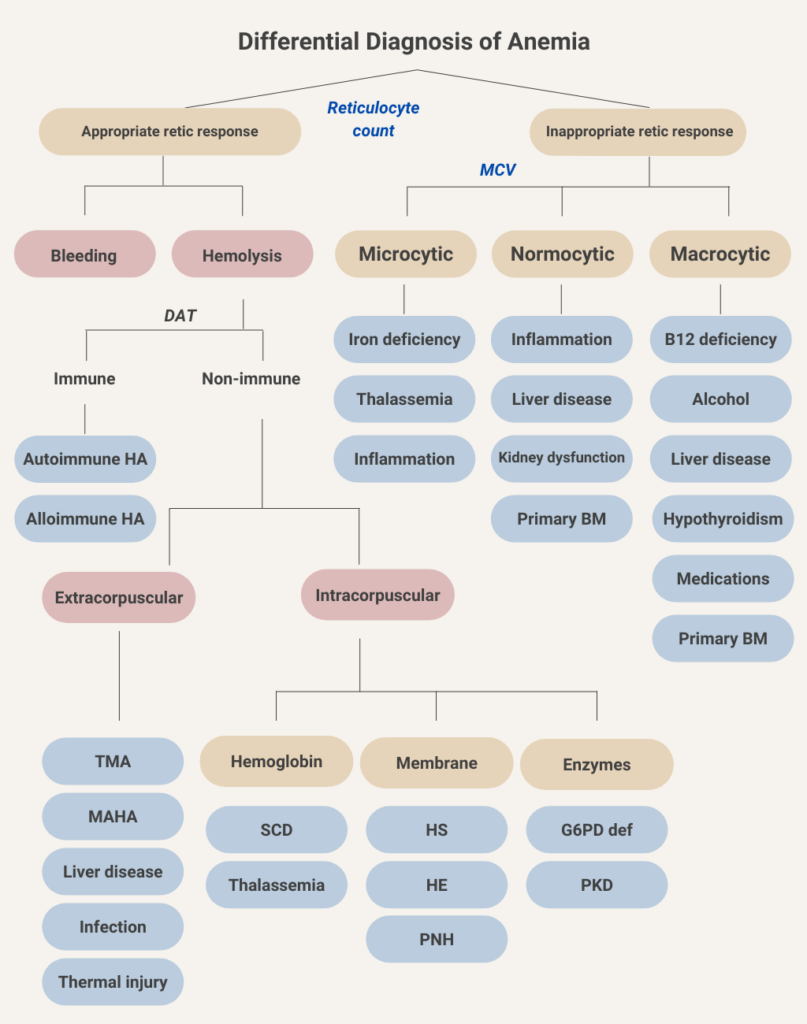
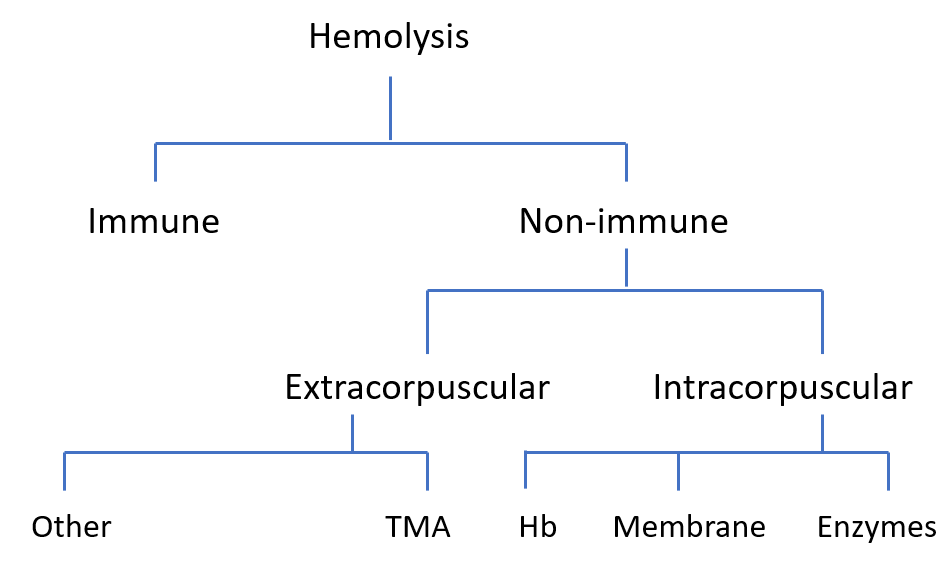
First branchpoint in diagnostic algorithm is immune vs. non-immune hemolysis. Virtually all cases of immune-mediated hemolysis (whether alloimmune or autoimmune) will be associated with a positive direct antiglobulin test (DAT) (Coombs test).
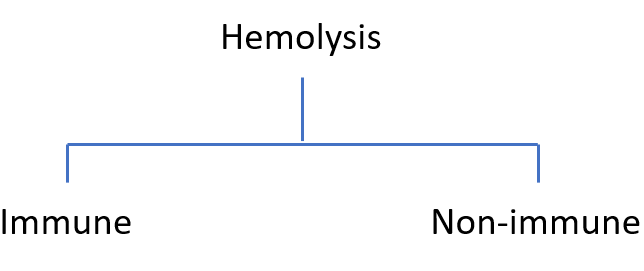
If the DAT is negative, the differential diagnosis includes extracorpuscular and intracorpuscular non-immune conditions. Extracorpuscular causes are those in which the red cells are innocent bystanders, reacting to changes in their extracellular environment. Intracorpuscular causes are those that are inherent in the red cell itself.
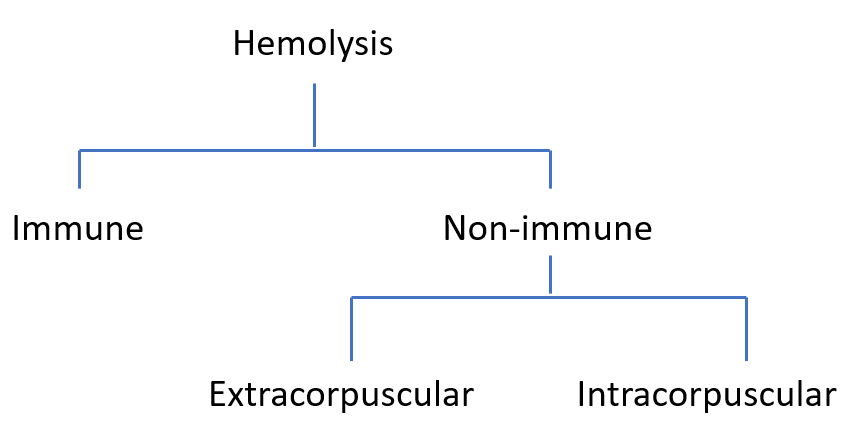
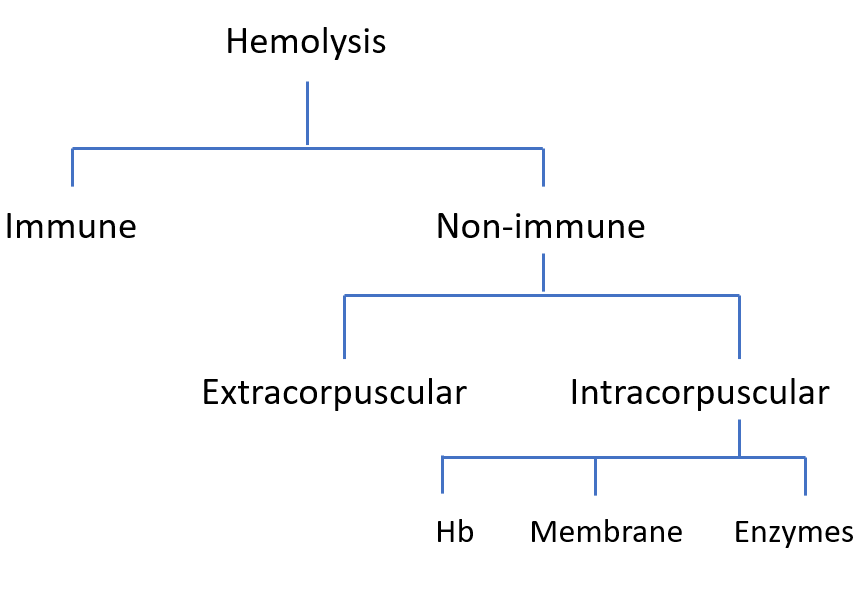
Intracorpuscular causes of hemolysis involve three broad categories: defects in hemoglobin, membrane or enzymes. The hemoglobin ‘bucket’ includes thalassemia and sickle cell disease; membrane causes include hereditary spherocytosis, hereditary elliptocytosis and hereditary stomatocytosis, and paroxysmal nocturnal hemoglobinuria (PNH; the only acquired condition in the intracorpuscular category); and defects in enzymes causing hemolysis include G6PD and pyruvate kinase deficiencies.
On the extracorpuscular side are conditions associated with thrombotic microangiopathy, including primary and secondary thrombotic thrombocytopenia purpura (TTP) and hemolytic uremic syndrome (HUS), and disseminated intravascular coagulation (DIC); and a series of non-TMA causes (“other”) including burns/thermal injury, microangiopathic hemolytic anemia from prosthetic valves or foot strike anemia, Clostridial sepsis, Wilson’s disease and spur cell anemia.