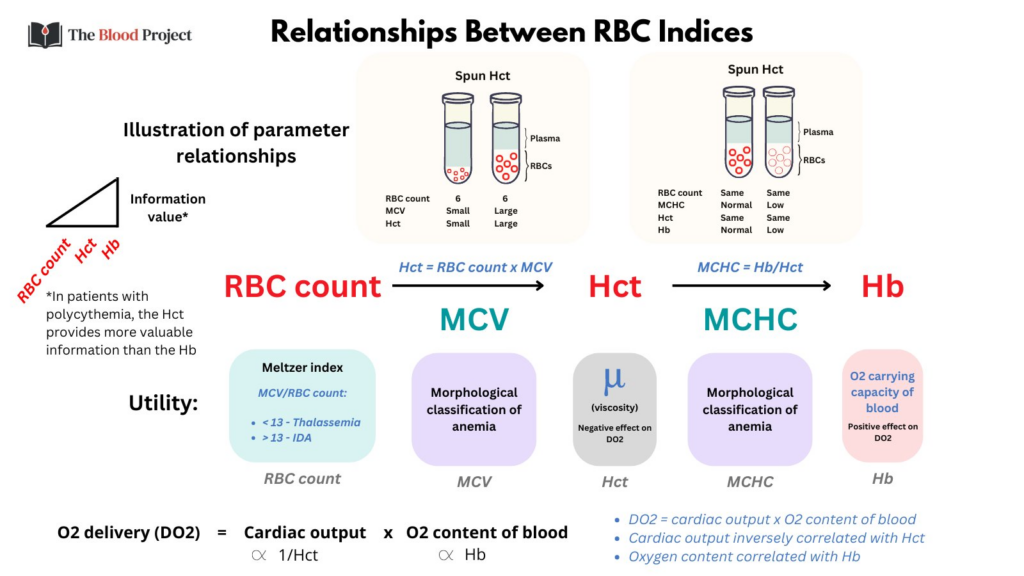
RBC count:
- Used to calculate the Hct (Hct = MCV x RBC count)
- Used by some to predict iron deficiency vs. thalassemia (e.g., Meltzer index)
- Largely ignored because it says nothing about the size/hemoglobinization of RBCs. Evolution has selected for an optimal Hb/Hct, not the RBC count (or MCV). One can achieved the same optimal Hct (viscosity) and Hb (oxygen carrying capacity) with many small cells or fewer large cells.
Mean cell volume (MCV):
- Very helpful because it is the first branch point in the differential diagnosis of anemia – microcytic vs. normocytic vs. macrocytic. Each has its own specific causes.
Hematocrit (Hct):
- The Hct is helpful to a point. As mentioned above it is calculated from the MCV and RBC count. Note that it is impervious to the content of the RBCs – they could contain Hb or cottage cheese for all the Hct cares.
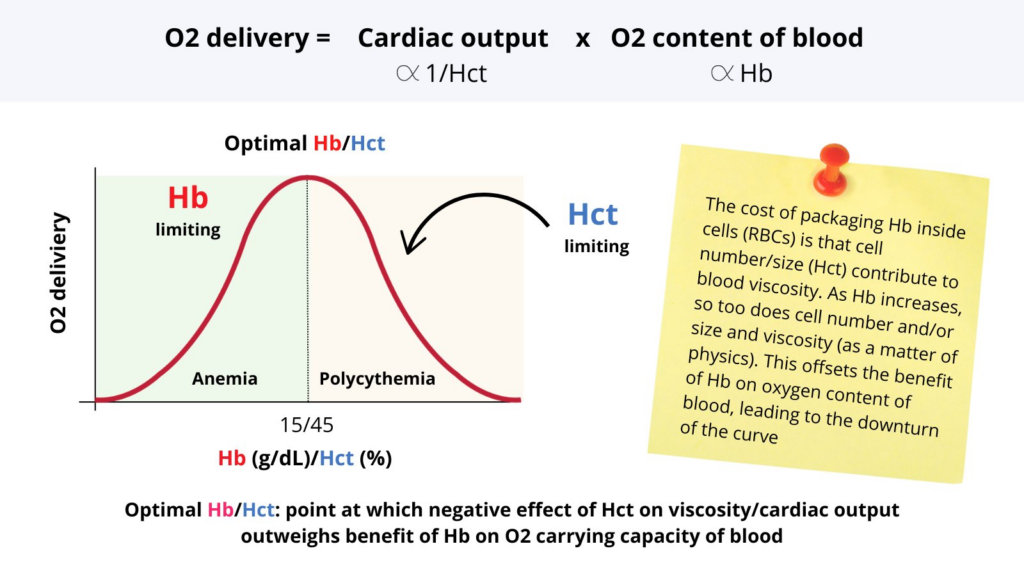
- The only time the Hct is useful is in patients with polycythemia where the negative effects of Hct on blood viscosity (and therefore total peripheral resistance and cardiac output) outweigh the benefits of Hb on oxygen content of blood.
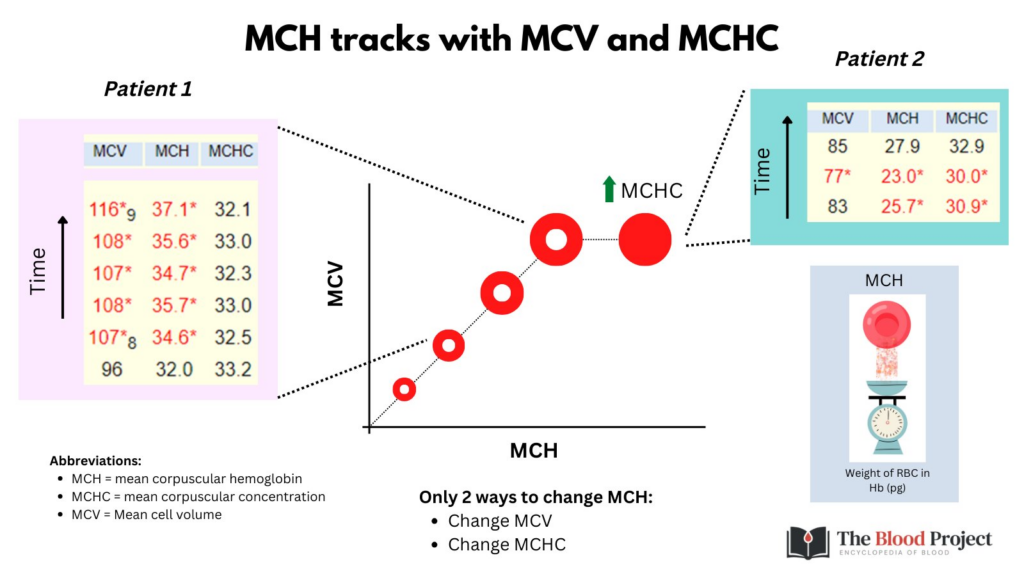
Mean corpuscular hemoglobin concentration (MCHC):
- Think about the MCHC as the degree of central pallor of the RBC – the more central pallor, the lower the MCHC. It is so much more useful than the MCH (which simply tracks with MCV and MCHC). The MCHC is the second branch point in the differential diagnosis of anemia. For example, microcytosis may be associated with a low MCHC (iron deficiency), normal MCHC (thalassemia trait) or increased MCHC (spherocytosis).
Hemoglobin:
- The crown jewel of the RBC parameters! Provides DIRECT information about the oxygen carrying capacity of blood (Hb x arterial oxygen saturation), and therefore oxygen delivery to the tissues.