“With the publication of a large, well-controlled, UK-based population study, strongly supported by another similarly large study from the USA, the risks of PPI-induced iron deficiency (ID) have been definitively established.”1
Hypochlorhydric states have long been known as an important cause of iron deficiency; such states include:
Atrophic gastritis
Partial gastrectomy
Medications, especially proton pump inhibitors (PPIs)
PPI-mediated iron deficiency:
PPIs are among the most commonly used pharmaceuticals in the United States. In 2012, 14.9 million patients received 157 million prescriptions for PPIs.
First report of PPI-associated iron deficiency published in 2002; described IDA induced by long-term usage of a PPI.
Mechanisms of PPI-associated iron deficiency:
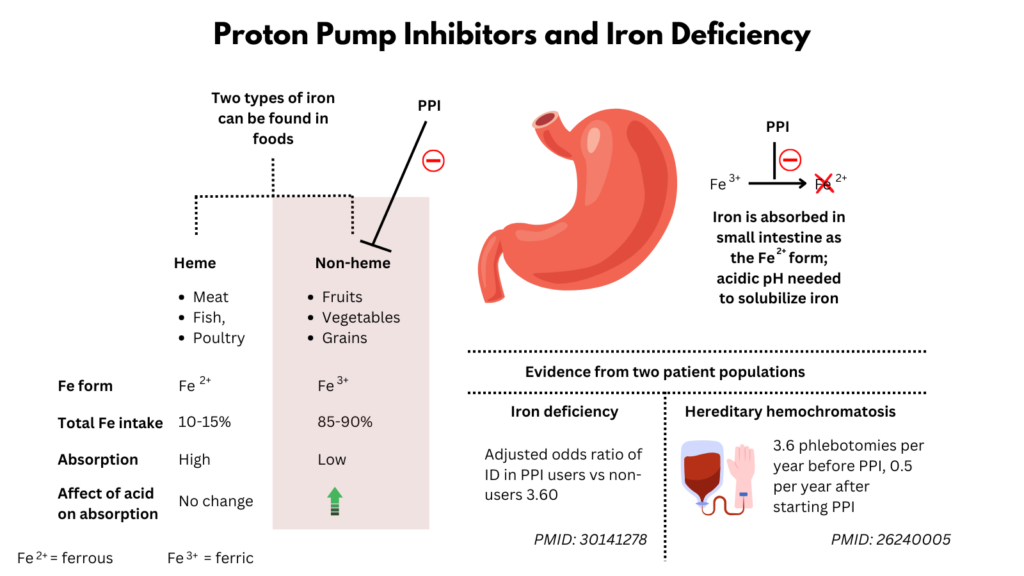
Dietary iron consists of both heme and non heme iron:
Heme iron:
Derived from the hemoglobin and myoglobin in animal food sources such as meat, seafood, and poultry.
Is in the ferrous (Fe2+) oxidation state.
Easily absorbable, largely uninfluenced by other dietary constituents.
Contributes to about 10%-15% of the total iron intake in individuals who consume meat.
Non-heme (or inorganic) iron:
Exists predominantly in the oxidized or ferric (Fe3+) form and is derived from plants and iron fortified food.
Highly insoluble.
Less well absorbed than heme iron.
Must be reduced to (Fe2+) before transport.
Bioavailability is influenced by many dietary components.
Gastric acid and ascorbic acid promote reduction and solubilization of dietary ferric iron and thus improve absorption.
Gastric acid has an important role in the release of non-heme iron, the major form of iron in most food.
Thus, PPIs which irreversibly inhibit the stomach’s H+/K+ ATPase proton pump within gastric parietal cells, can lead to iron malabsorption.
A case–control study involving the analysis of community repeat prescriptions among subjects referred with IDA, and unmatched controls referred as gastroenterology fast-tracks for other indications.
409 subjects in the IDA group and 801 in the control group
Significant associations were identified between presentation with IDA and long-term exposure to PPIs (OR 3.29, 95% CI: 2.47 to 4.41, p<0.001).
Conclusions: Long-term exposure to PPIs is independently associated with the risk of developing IDA.
77,046 cases of patients with new iron deficiency and 389,314 controls.
Cases were more likely than controls to have been dispensed a >2-year supply of PPIs (3.0% vs 0.9%).
A new iron deficiency diagnosis was over twice as common among persons with a >2-year prior supply of PPIs than among nonusers.
There was a significant dose trend.
Among persons taking PPIs for >2 years, the highest mean daily dose was more strongly associated with iron deficiency (>1.5 PPI pills/d: OR, 2.61; 95% CI, 2.27-3.01) than the lowest dose (<0.75 PPI pills/day)
The risk of iron deficiency increased with longer durations of use across all users.
Conclusions: Among patients without known risk factors for iron deficiency, gastric acid inhibitor use for >2 years was associated with an increased subsequent risk of iron deficiency. The risk increased with increasing potency of acid inhibition and decreased after medication discontinuation.
Cases were patients aged 19 years or older with first-time diagnosis of ID between 2005 and2016 (n = 26 806).
Among cases:
2960 were PPI “full” users who had received PPIs for a continuous duration of at least 1 year prior to the index date (PFU).
6607 were “limited” users (subjects who intermittently received PPI therapy; PLU).
17,239 were PPI non-users (subjects who received no PPI prescriptions prior to the index date; PNU).
Among controls:
1091 were PFU
5058 PLU
20,657 PNU
Adjusted odds ratio of ID in PFU and PLU compared to PNU was 3.60 (95%CI, [3.32–3.91]) and 1.51 (95% CI, [1.44–1.58]).
Positive dose–response and time–response relationships were observed.
Conclusions: Chronic PPI use increases the risk of ID. Physicians should consider this when balancing the risks and benefits of chronic PPI prescription.
Retrospective study of patients with HH homozygous for the C282Y mutation b
In a paired group analysis of 12 patients, the authors compared mean serum levels of ferritin and number of phlebotomies needed each year during the periods of 3 years before and 3 years after the start of PPI therapy.
The authors compared these results with those from a group who received PPIs for at least 2 years (n = 9) and a group who never received PPIs (n = 36).
Significant reduction in median number of phlebotomies after patients began taking PPIs vs before (0.50 vs 3.17, P < .002).
Patients who received PPIs for at least 2 years needed significantly fewer phlebotomies than patients in the paired group before they started taking PPIs (1.25 vs 3.17, P < .001).
The number of phlebotomies in the group who never received PPIs was significantly higher than in the paired group after they started taking PPIs (3.0 vs 0.5, P < .001).
Conclusions: On the basis of a retrospective analysis, in patients with HH homozygous for the C282Y mutation in HFE, treatment with PPIs for 2 or more years significantly reduced the number of phlebotomies required to maintain serum levels of ferritin below 100 mg/L.
30 p.C282Y homozygous patients were randomly allocated to PPI (pantoprazole 40 mg/day) or placebo for 12 months.
Phlebotomies were performed when serum ferritin was > 100 mg/L.
Phlebotomy need turned out to be significantly lower in patients taking PPI (P = .0052).
PPI treatment significantly reduces the need for phlebotomies in p.C282Y homozygous patients. In view of the known long-term safety profile of PPI, they can be a valuable addition to standard therapy.
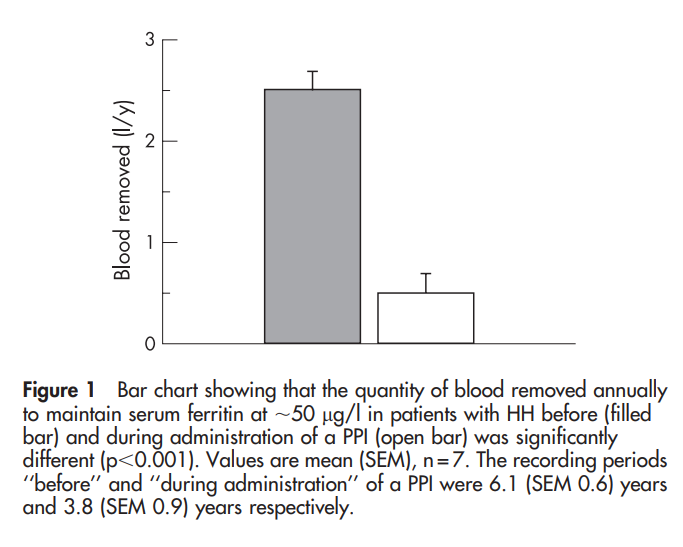
Phlebotomy requirements to keep serum ferritin about 50 mg/l before (mean 6.1 (SE 0.6) years) and during (3.8 (0.9) years) administration of a PPI were evaluated in seven patients and a post-prandial study was performed to determine whether PPIs reduce absorption of non-haem iron (14.5 mg) from a test meal in a further 14 phlebotomized patients with normal iron stores.
There was a significant reduction (p < 0.001) in the volume of blood removed annually before (2.5 (0.25) l) and while taking (0.5 (0.25) l) a PPI.
Administration of a PPI for 7d suppressed absorption of non-haem iron from the meal as shown by a significant reduction (all p < 0.01) in:
Area under the serum curve (2145 (374) versus 1059 (219))
% recovery of administered iron at peak serum iron (20.5 (3.2) versus 11.0 (2.0)%)
Peak serum iron (13.6 (2.4) vs 6.1 (1.2) mmol/l)
Conclusions: Administration of a PPI to patients with HH can inhibit the absorption of non-haem iron from a test meal and the habitual diet.
Treatment of PPI-associated iron deficiency:
Stop the PPI
Switch to an H 2-receptor antagonist (less risk of ID)
British Society of Gastroenterology (BSG) guideline on the management of iron deficiency anaemia in adults:
“More recently it has been recognised that long-term proton pump inhibitor (PPI) therapy may contribute to the risk of iron deficiency, presumably as a result of impaired absorption secondary to hypochlorhydria… Iron deficiency is however often multifactorial, and so the presence of one or more of these risk factors should not necessarily be a deterrent to further GI investigation, particularly in older age groups.”
American College of Gastroenterology (ACG) guideline on hereditary hemochromatosis:
The results of these studies (referring to the three studies above) imply that PPIs could have an additional role in the treatment of selected patients with HH to reduce the frequency of phlebotomies. Nonetheless, we do not recommend the routine use of PPIs as a treatment in HH. However, if they are otherwise needed for other primary indications, they may have the benefit of reducing the frequency of phlebotomies needed.
We recommend against the routine use of PPIs as the primary treatment of HH (strong recommendation, low quality of evidence).