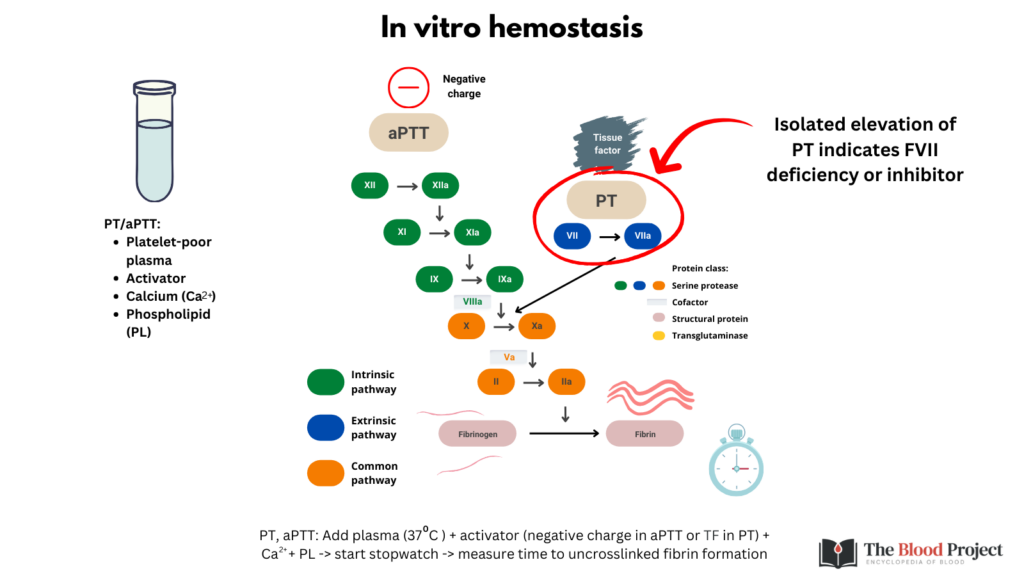
What causes an isolated elevation in the PT?
From a mechanistic standpoint: an inhibitor against or deficiency of FVII in the extrinsic pathway.
From a practical standpoint: warfarin, liver disease, disseminated intravascular coagulation (DIC) and vitamin K deficiency, each of which also affects the intrinsic and common pathways (congenital FVII deficiency is far less common).
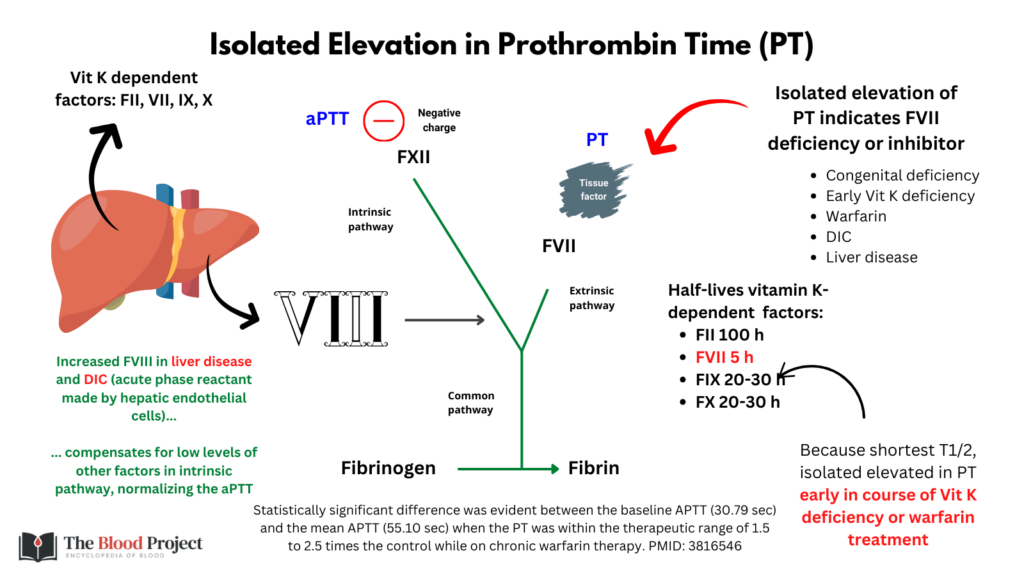
How do we reconcile the observation that the the most common causes of isolated elevation in PT also affect factors in the intrinsic pathway and should therefore increase the aPTT as well?
The following are possible explanations:
- Vitamin K antagonists cause an isolated elevation of PT early in the course of treatment because FVII has the shortest half-life of the vitamin K-dependent factors.
- With chronic therapy/vitamin K deficiency, all vitamin K dependent factors are at equilibrium and though we may not always notice it, the aPTT is also prolonged.
- In DIC and liver disease, there is increased production of the acute phase reactant, FVIII, by liver sinusoidal endothelial cells. This may compensate for the reduction of other intrinsic pathway factors, normalizing the aPTT.