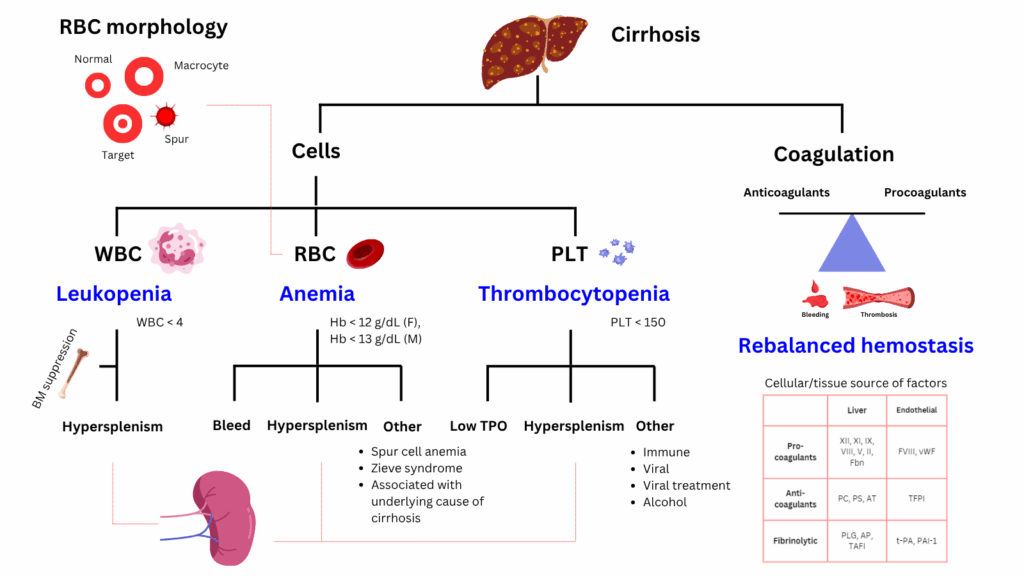
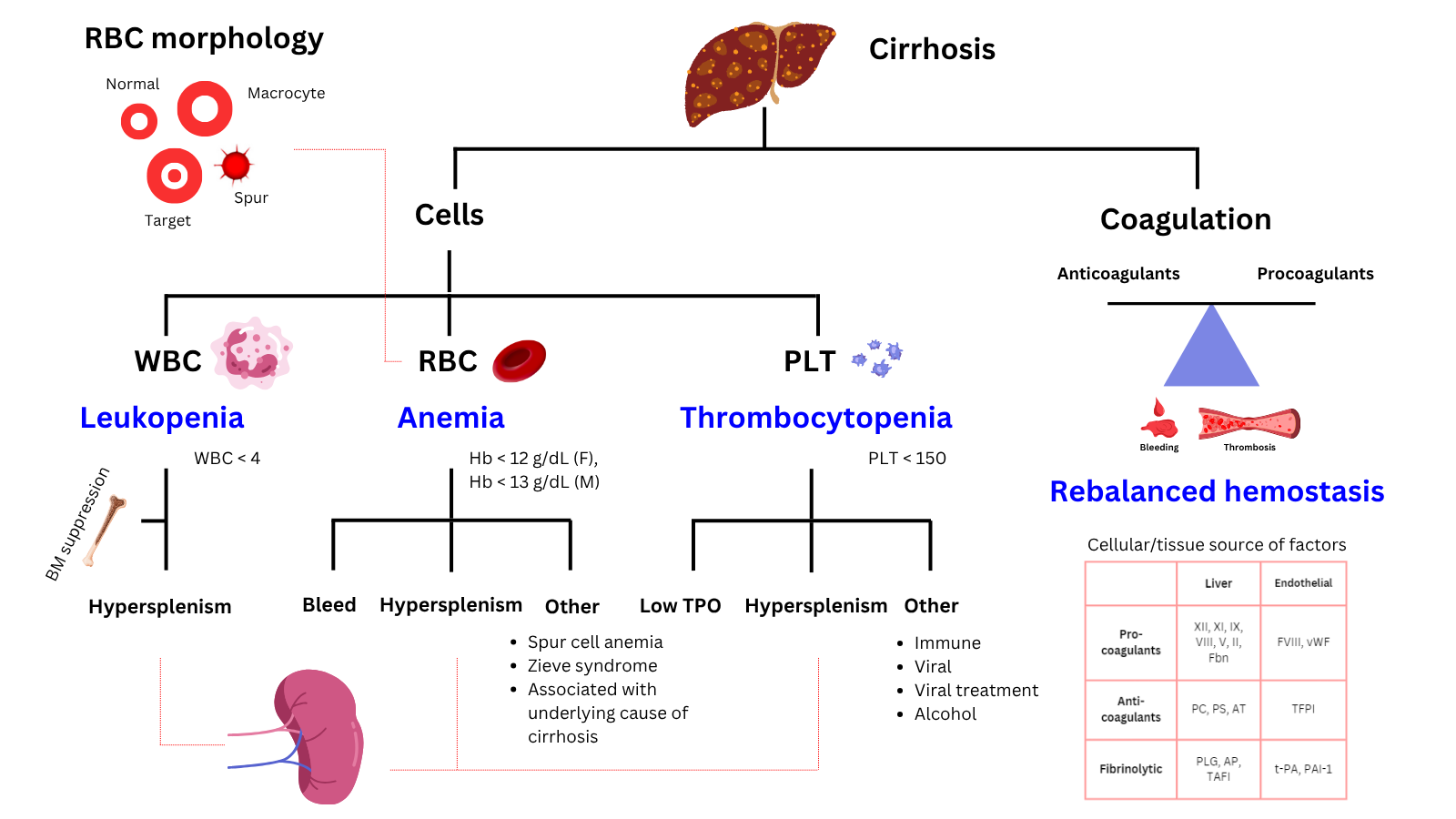
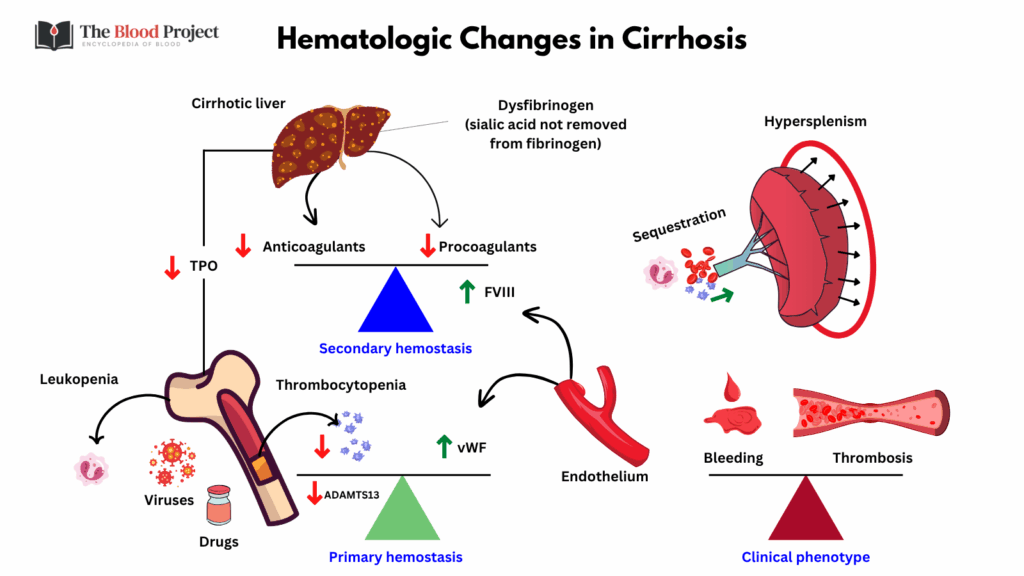
Cirrhosis, a condition marked by chronic liver damage and architectural distortion, has widespread hematologic effects due to portal hypertension, hypersplenism, impaired liver synthetic function, and altered immune regulation. The hematological manifestations of cirrhosis are primarily thrombocytopenia, anemia, and leukopenia. Thrombocytopenia is the most common, resulting from splenic sequestration due to portal hypertension, decreased hepatic synthesis of thrombopoietin, and increased platelet destruction. Anemia arises from chronic gastrointestinal blood loss (often from varices), nutritional deficiencies, hypersplenism, and bone marrow suppression. Leukopenia, particularly neutropenia, is also seen and is mainly due to hypersplenism and bone marrow suppression.
Cirrhosis also causes complex alterations in hemostasis, with decreased synthesis of both procoagulant and anticoagulant factors, leading to a rebalanced but fragile hemostatic state. Patients may have prolonged prothrombin time (PT) and elevated international normalized ratio (INR), but these do not reliably predict bleeding risk. There is also increased von Willebrand factor and decreased ADAMTS13, contributing to a prothrombotic tendency despite traditional markers suggesting hypocoagulability. The American Association for the Study of Liver Diseases highlights that both bleeding and thrombotic complications can occur, and that routine coagulation tests do not fully capture the hemostatic balance in cirrhosis.
For larger image, click here.
{kind=link}
For larger image, click here.
{kind=link}
Red blood cells
- Anemia
- Typically normocytic, but also macrocytic (due to liver disease, alcohol, B12 or folate deficiency) or microcytic (iron deficiency)
| Type | Mechanism |
|---|---|
| Anemia of chronic disease | Hepcidin-mediated iron sequestration and decreased erythropoiesis |
| Iron-deficiency anemia | GI bleeding (e.g., varices, portal hypertensive gastropathy, ulcers) |
| Hemolytic anemia | Hypersplenism*; spur cell anemia in advanced liver disease; copper mediated hemolysis in Wilson disease |
| Megaloblastic anemia | Folate deficiency (common in alcohol-related liver disease) |
| Aplastic or toxic anemia | Alcohol-induced marrow suppression |
- Other RBC findings:
- Target cells (due to liver dysfunction)
- Acanthocytes/spur cells (severe liver disease; associated with hemolysis)
- Macrocytosis (alcohol use, folate deficiency, or reticulocytosis)
White blood cells
| Feature | Mechanism |
|---|---|
| Leukopenia/neutropenia | Hypersplenism (sequestration), bone marrow suppression (alcohol, viruses) |
| Impaired immune function | Dysfunctional neutrophils and monocytes |
Platelets
- Thrombocytopenia
- Most common and earliest hematologic abnormality in cirrhosis
- Seen in up to 78% of cirrhotics
| Cause | Mechanism |
|---|---|
| Hypersplenism | Sequestration of platelets in enlarged spleen |
| Decreased thrombopoietin | Reduced synthesis by diseased liver |
| Bone marrow suppression | Alcohol, hepatitis viruses |
Coagulation
Despite an elevated INR, patients with cirrhosis are in a rebalanced but fragile hemostatic state.
| Finding | Mechanism |
|---|---|
| Prolonged PT/INR, aPTT | Decreased synthesis of clotting factors (II, V, VII, IX, X) |
| Low fibrinogen (late) | Reduced synthesis in advanced liver failure |
| Low protein C, S, antithrombin | Natural anticoagulants reduced |

Miscellaneous Hematologic Findings
| Finding | Mechanism |
|---|---|
| Elevated ferritin | Inflammation, iron overload (especially with transfusions) |
| Elevated bilirubin | Impaired conjugation and excretion |
| Low B12 and folate | Poor synthetic liver function |