
For larger image, click here.
{kind=link}
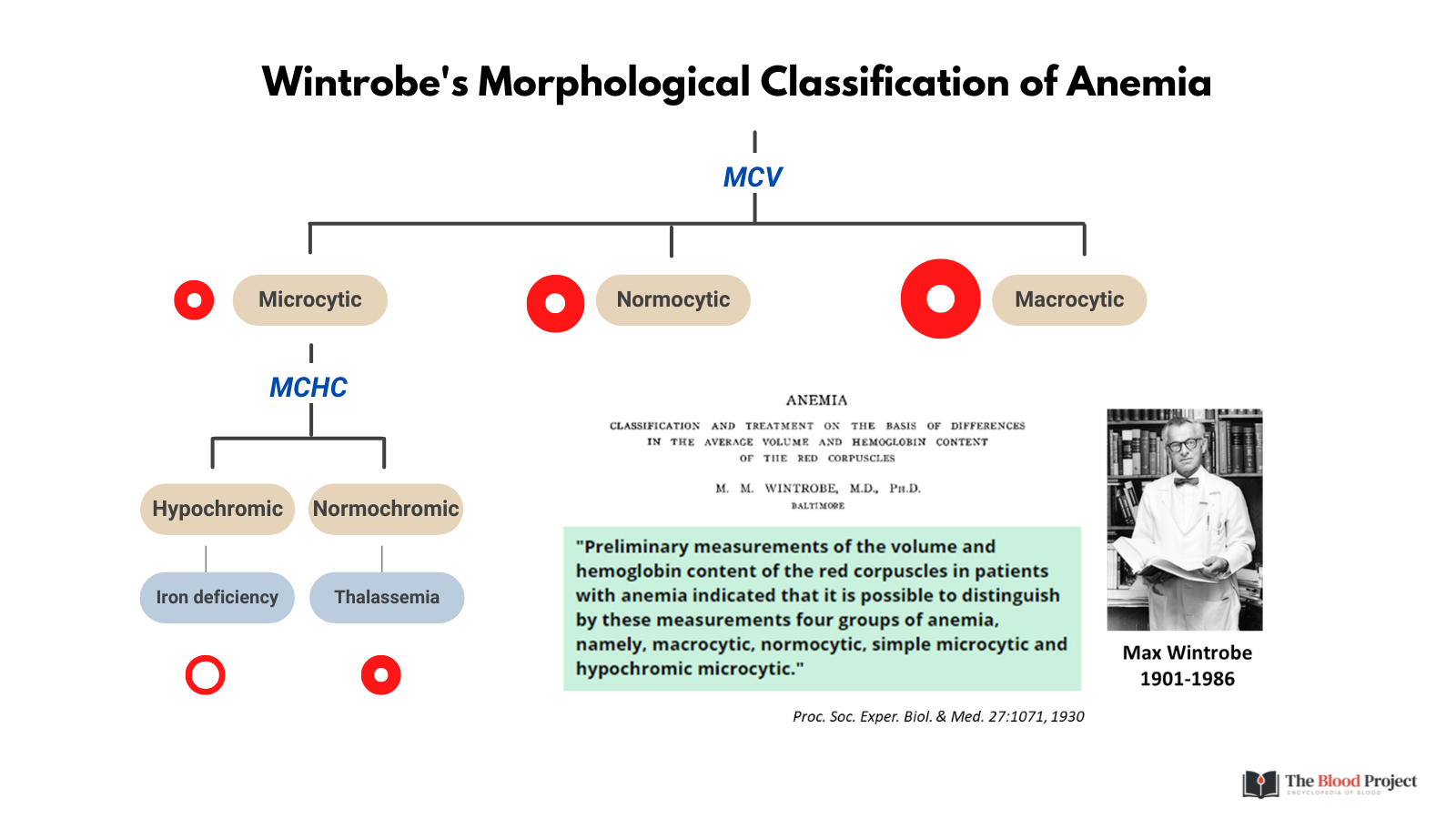
The classification of anemia is most commonly based on morphology, a system described initially by Maxwell Wintrobe. This morphological classification begins with an assessment of the mean corpuscular volume (MCV) to categorize anemia as microcytic, normocytic, or macrocytic, a key first branch point. A secondary branch point involves the mean corpuscular hemoglobin concentration (MCHC), which helps determine whether the anemia is hypochromic, normochromic, or hyperchromic (click here for a graphic). In parallel or as a next step, the reticulocyte count plays a central role in evaluating whether the bone marrow response is appropriate for the degree of anemia. The reticulocyte count can be measured at the same time as the CBC, allowing the red cell indices (MCV, MCHC) to be interpreted in the context of marrow responsiveness. Alternatively, clinicians may first assess the MCV and MCHC before ordering a reticulocyte count, especially in initial evaluations. Either way, the integration of morphologic indices with reticulocyte data provides a powerful framework for distinguishing between hypoproliferative and hyperproliferative causes of anemia.
{kind=link}
An alternative framework is the functional or mechanistic classification, which mirrors the approach used in thrombocytopenia. It divides anemia into categories of:
- Hemodilution:
- Blood loss followed by IV fluids or fluid shifts from extravascular to intravascular space.
- Excessive fluid administration1
- Pregnancy
- Underproduction:
- Anemia due to underproduction of red cells can result from:
- Nutritional deficiencies (iron, copper, vitamin B12, folate)
- Erythropoietin deficiency, commonly seen in chronic kidney disease
- Bone marrow failure (e.g., red cell aplasia, marrow infiltration)
- Chronic inflammation or infection
- Anemia due to underproduction of red cells can result from:
- Increased destruction:
- This includes:
- Peripheral hemolysis, with its own subcategories:
- Immune vs. non-immune
- Intravascular vs. extravascular
- Ineffective erythropoiesis, such as in megaloblastic anemia or myelodysplasia
- Marrow destruction or consumption, e.g., in hemophagocytic lymphohistiocytosis (HLH)
- Peripheral hemolysis, with its own subcategories:
- This includes:
- Sequestration
- While splenic sequestration is often cited as a cause of anemia, its role is more complex. In thrombocytopenia, splenic pooling leads to a redistribution of platelets, but total platelet mass remains unchanged. The thrombopoietin (TPO) feedback system senses total mass, not location, so there is no compensatory increase in platelet production.
- In contrast, erythropoiesis is driven by oxygen delivery to the peritubular cells of the kidney. If red cells are sequestered in the spleen and oxygen delivery is reduced, erythropoietin production increases, leading to compensatory red cell production—unless the bone marrow cannot respond (e.g., in chronic kidney disease). Therefore, unless EPO production is inadequate or erythropoietic response is blunted, splenic sequestration alone does not typically result in anemia.
Operational utility of each classification:
- The morphological classification is practical and widely used, especially in the initial evaluation of anemia in the clinical setting. It is particularly valuable when the reticulocyte count is low, guiding a structured approach based on red cell size and hemoglobin content.
- The functional classification, while valuable from a conceptual and teaching perspective, is less actionable at the bedside. It is analogous to the approach used in thrombocytopenia, but whereas most thrombocytopenia reflects destruction/consumption, the causes of anemia are more diverse and nuanced.
- In summary, both the morphological and functional classifications are helpful, but serve different purposes. The former is more practical in clinical workflows, while the latter promotes deeper mechanistic understanding. Used together, they provide a more complete framework for evaluating patients with anemia.