Vitamin B12
Vitamin B12 (cobalamin) is an essential water-soluble vitamin required for red blood cell production, DNA synthesis, and neurologic function. It is found naturally in animal-based foods and has a complex absorption pathway involving intrinsic factor and the terminal ileum. Deficiency can lead to megaloblastic anemia and neurologic complications, while elevated levels may signal underlying liver disease or malignancy.
Overview of vitamin B12:
- Also known as cobalamin
- A water-soluble vitamin essential for:
- DNA synthesis
- Neurological function
- Red blood cell production
- Found only in animal-derived foods (meat, dairy, eggs); not present in plants
- Daily requirement: ~2–3 µg/day
- Body stores: 2–5 mg, mostly in the liver (sufficient for 2–5 years)
Absorption Pathway:
- In the mouth/stomach:
- B12 is protein-bound in food
- Stomach acid and pepsin release B12 from food proteins
- B12 binds to haptocorrin (also called R-binder or transcobalamin I) secreted by salivary glands and gastric mucosa
- In the small intestine:
- In the duodenum, pancreatic proteases degrade haptocorrin
- Free B12 then binds to intrinsic factor (IF), a glycoprotein secreted by gastric parietal cells
- The B12–IF complex travels to the terminal ileum, where it binds to cubilin receptors and is absorbed via receptor-mediated endocytosis1
- In the enterocyte and bloodstream:
- Inside enterocytes, B12 dissociates from IF
- It binds to transcobalamin II (TCII) for systemic transport
- Only B12–TCII complex (called holotranscobalamin) is biologically active and taken up by tissues
Storage and transport:
- B12 is stored in the liver (main site), but also in muscle
- Transcobalamin II transports active B12 to tissues. It carries about one quarter of vitamin B12 in serum
- Transcobalamin I (haptocorrin) and III bind inactive or circulating B12 pools2
More about the transcobalamins:
- TCB I and III:
- 60–70kDa molecular weight proteins
- Belong to the haptocorrin (HC) superfamily
- HCs, also called R-binders or cobalophilins, are found in various tissues and biological fluids
- TCB I and III are derived from the granulocyte line and are markers of neutrophilic secondary granules, which explains their increase in myeloproliferative disorders (MPDs).
- TCB II:
- 42–47kDa protein
- Essential protein in the delivery of vitamin B12 to cells and tissues
- The production site of TCB II is primarily hepatocytic, and secondarily endothelial, monocytic and intestinal
Functions of vitamin B12:
- B12 acts as a cofactor for two key enzymatic reactions:
- Methionine Synthase (cytoplasm):
- Converts homocysteine → methionine
- Requires methylcobalamin
- Supports DNA synthesis via the folate cycle (regenerates tetrahydrofolate)
- Methylmalonyl-CoA Mutase (mitochondria):
- Converts methylmalonyl-CoA → succinyl-CoA
- Requires adenosylcobalamin
- Involved in fatty acid and amino acid metabolism
- Methionine Synthase (cytoplasm):
Elevated vitamin B12 (hypervitaminemia B12)
While vitamin B12 deficiency is commonly discussed, elevated serum B12 (hypercobalaminemia) is less common and often overlooked or misinterpreted. An elevated vitamin B12 level often reflects increased intake (oral supplementation, recent intramuscular injection) or high dietary consumption, especially from fortified foods or animal products. However, it may reflect underlying disease.
Definition:
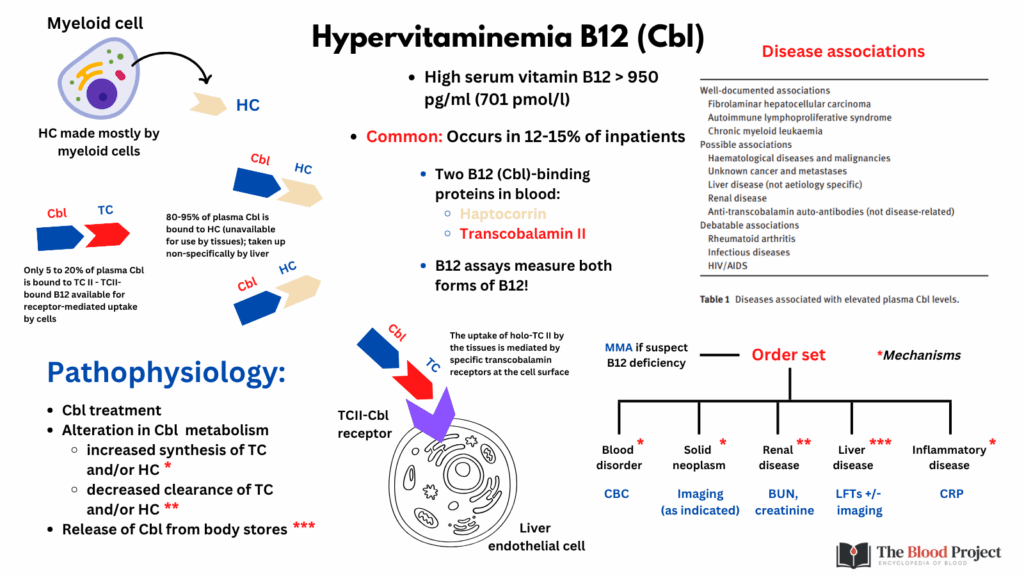
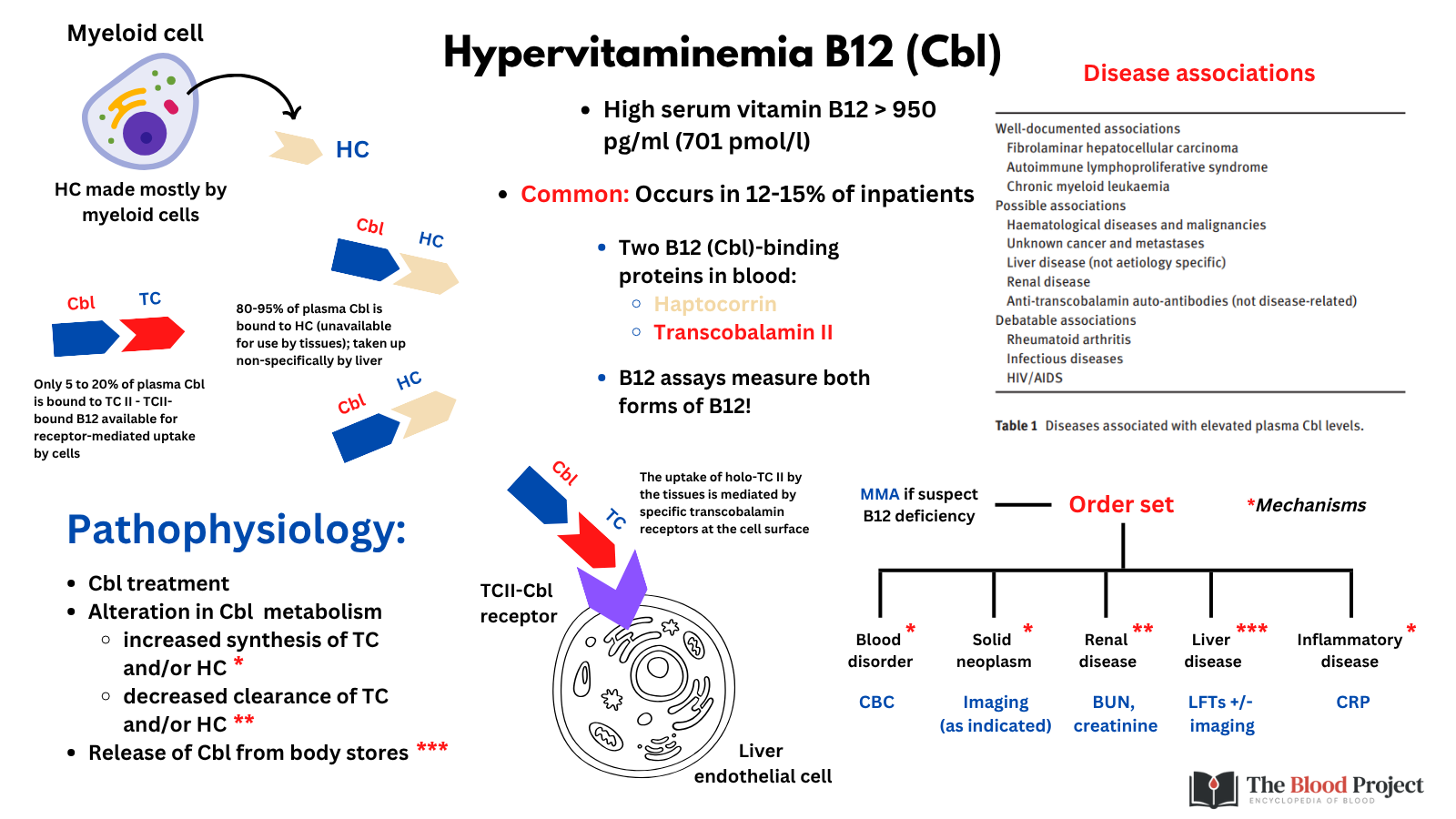
- High serum vitamin B12 is defined by a rate above 950 pg/ml (701pmol/l), which corresponds by biological standards, to the upper limit of biological normality.
Epidemiology:
- High levels of vitamin B12 were found in:
Causes:
- Excessive supplementation (a direct increase in plasma vitamin B12 by excess intake or administration)
- Increased release of vitamin B12 from tissue stores (liberation from an internal reservoir):
- Solid tumors (especially hepatic or hematologic malignancies)
- Liver metastases
- Increased binding proteins:7
- Excess production:
- Liver disease (e.g., hepatitis, cirrhosis, hepatocellular carcinoma) – damaged hepatocytes release haptocorrin (transcobalamin I) and B12 into circulation
- Myeloproliferative disorders – these increase granulocyte production, which leads to more haptocorrin (transcobalamin I/III), a B12-binding protein produced by proliferating myeloid cells.
- Inflammation – haptocorrin levels can increase due to granulocyte activation or as an acute phase response
- Decreased clearance:
- Renal failure – decreased clearance of transcobalamin–B12 complexes
- Excess production:
Mechanism:
- Most elevated B12 is not free or biologically active, but rather bound to haptocorrin, which has a long half-life and is increased in certain diseases.
- Therefore, total serum B12 may be high, but active B12 (holotranscobalamin) may be normal.
Clinical significance:
- Persistent elevation (>1000 pg/mL) without supplementation should prompt further evaluation.
- May be a marker of underlying disease (e.g., liver disease, malignancy, MDS/CML).
- Interpretation should consider:
- Symptoms
- CBC (especially if basophilia, leukocytosis, etc.)
- Liver function tests
- Renal function
- Inflammatory markers
- Even high serum cobalamin levels can be accompanied by functional deficiency
Suggested Workup for Unexplained High B12:
- Repeat B12 measurement off supplements
- Check:
- Liver enzymes
- CBC with differential
- Serum creatinine
- Holotranscobalamin – active fraction of vitamin B12, bound to TCB II8
- Consideration of myeloproliferative neoplasm workup if hematologic abnormalities are present
- Imaging if malignancy suspected (e.g., abdominal imaging if liver pathology or malignancy is suspected)
In summary, while elevated B12 is most often benign and related to supplementation or liver/renal dysfunction, it is essential to rule out underlying hematologic malignancy or solid organ cancer when unexplained or accompanied by abnormal clinical or laboratory findings.
For larger image, click here.
{kind=link}