How expert consultants define terrain, assign weight, and make judgment visible when laboratory markers suggest red cell destruction and stakes are real
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
More Than a Number: When Hemoglobin Becomes a Physiologic Threshold
Severe anemia is not just a low laboratory value.
It is a signal that a patient may be approaching — or crossing — a physiologic threshold.
The same hemoglobin can live in very different clinical worlds:
- a chronically anemic patient with preserved adaptation
- a patient with acute blood loss
- a patient with evolving hemolysis
- a patient with marrow failure
- a patient whose reserve is limited by cardiopulmonary disease
In each case, the number may be identical.
The danger is not.
This is why severe anemia is not primarily a diagnostic problem.
It is a reserve and threshold judgment problem.
Expert consultation is not about naming a cause as quickly as possible.
It is about recognizing physiologic risk, defining urgency, and adapting posture as the biology declares itself.
Consult Practice makes that expert judgment visible.
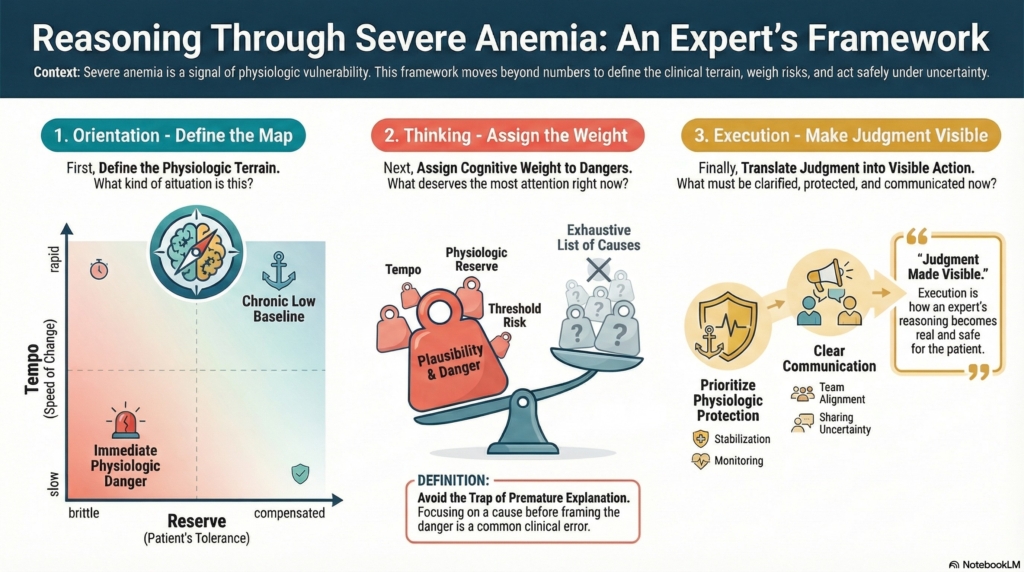
The three-layer framework: Orientation, Thinking, Execution
This series approaches suspected hemolysis through three distinct cognitive layers:
- Orientation — defining the terrain
- Thinking — assigning weight within that terrain
- Execution — making judgment visible through action and communication
Each layer has a different job.
Confusing them is one of the most common sources of clinical error.
Orientation defines the map
Orientation answers a simple but powerful question:
What kind of physiologic world am I in right now?
Orientation is not diagnosis.
It is terrain definition.
In severe anemia, Orientation clarifies:
- how dangerous this hemoglobin might be for this patient
- how fast physiology may deteriorate
- how much uncertainty can be safely tolerated
- whether this represents acute loss, chronic adaptation, or evolving instability
Orientation helps distinguish between terrains such as:
- immediate physiologic danger
- chronic compensated anemia
- bleeding-dominant physiology
- marrow or multi-lineage failure
- evolving pictures requiring surveillance
These are not causes.
They are problem spaces.
Orientation often begins at the time of the page, but it is not a one-time act.
Whenever new information changes the nature of the situation, Orientation is re-invoked.
Orientation answers:
What kind of situation is this?
Thinking assigns weight within the defined world
Once the terrain is defined, Thinking takes over.
Thinking answers a different question:
Within this world, which dangers and explanations deserve the most cognitive weight right now?
This is not about listing every cause of anemia.
It is about plausibility-weighting under uncertainty.
Thinking in severe anemia focuses on:
- tempo
- physiologic reserve
- threshold risk
- and consequence
Expert consultants use Thinking to:
- recognize when hemoglobin has become a reserve-threat
- distinguish acute loss from chronic underproduction
- hold multiple explanations provisionally
- avoid premature explanation
- recalibrate weight as trajectory evolves
Thinking answers:
What deserves the most attention right now, and what would change that?
Execution makes judgment visible
Execution is where judgment becomes real to others.
Execution answers:
What must be clarified, protected, communicated, deferred, and revisited — right now?
This is where:
- physiologic stabilization is prioritized
- monitoring is made explicit
- uncertainty is communicated safely
- and recalibration is visible over time
Execution is not running a checklist.
It is translating judgment into safe clinical behavior.
Execution includes:
- first safety passes
- stabilization based on reserve and threshold
- tempo-based reassessment
- visible restraint when appropriate
- protective escalation when necessary
- transparent revision as biology evolves
Execution is best described as:
Judgment made visible.
Execution answers:
How does expert judgment look in real clinical time?
Why this framework matters in Severe Anemia
Many clinical errors in severe anemia do not arise from lack of knowledge.
They arise from:
- treating hemoglobin as a diagnosis
- reflexive transfusion without considering chronic adaptation
- premature explanation before physiology is framed
- failure to recognize sentinel severity as a danger signal
- or misjudging reserve and tempo
This framework protects against category failure:
- treating reserve-threat problems like diagnostic puzzles
- treating chronic adaptation like acute loss
- treating uncertainty as something to eliminate rather than manage
By separating Orientation, Thinking, and Execution, the consultant:
- defines the correct terrain
- assigns weight deliberately
- and makes judgment visible and adaptable
This is how expert consultants manage risk when facts are incomplete and stakes are real.
How to use this series
This overview is the conceptual front door.
The three companion essays go deeper:
- Orientation — for defining the physiologic problem space
- Thinking — for threshold- and reserve-based plausibility weighting
- Execution — for visible stabilization, communication, and recalibration
They are designed to be used together.
Not as algorithms.
Not as diagnostic manuals.
But as a guide to how expert consultants think, act, and revise posture in real clinical environments.
Bottom line
Severe anemia in hospitalized patients is not a diagnosis.
It is a signal of physiologic vulnerability.
Expert care depends on:
- defining what kind of physiologic world the patient is in
- assigning cognitive weight based on reserve and threshold
- and making judgment visible through safe, adaptive execution
Orientation defines the map.
Thinking assigns weight.
Execution makes judgment visible.
That is how hematologists reason when hemoglobin is critically low and the stakes are real.