Case
For larger image, click here.
{kind=link}
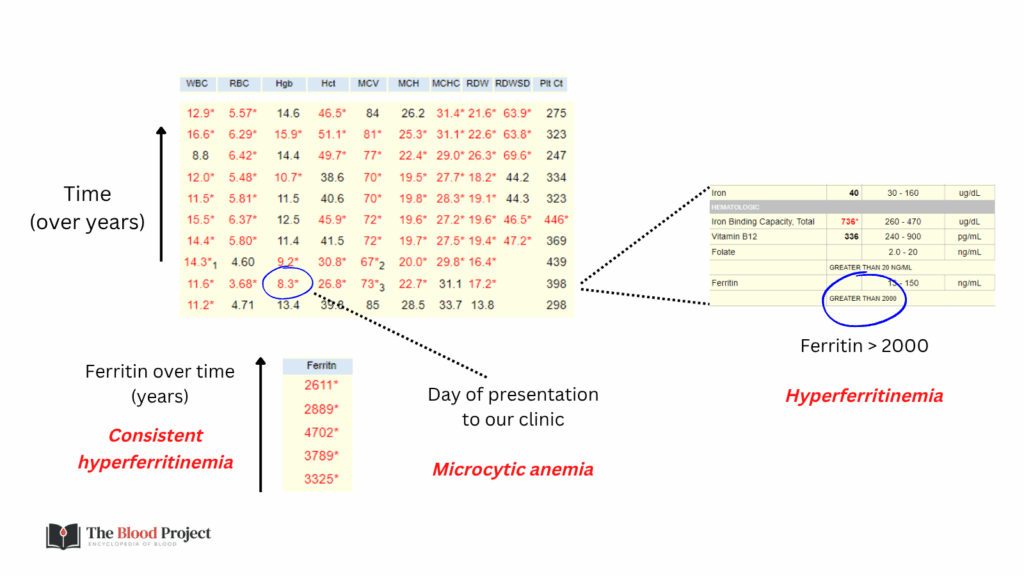
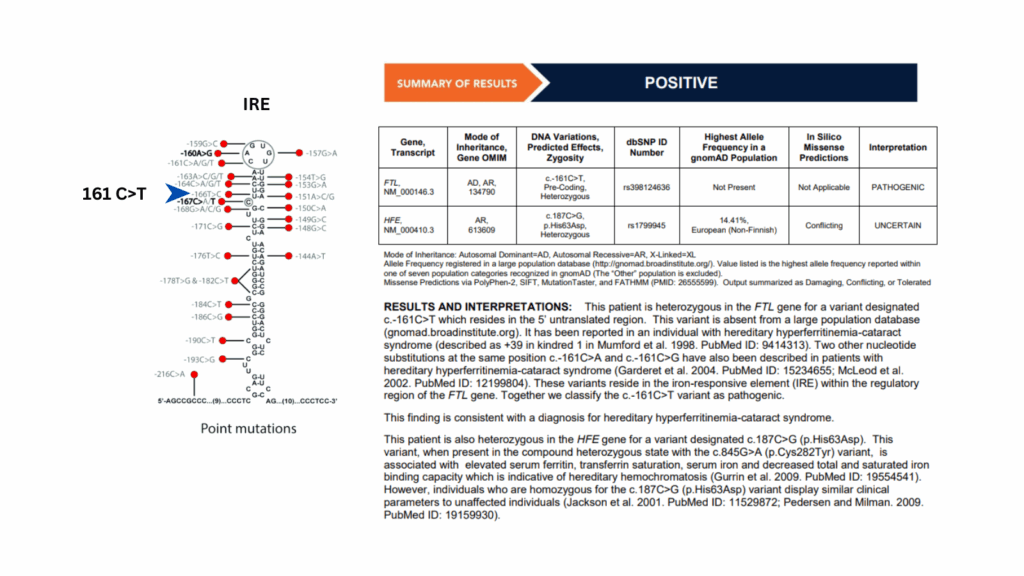
The above data are from a 52-year-old woman with a longstanding history of elevated serum ferritin and bilateral cataracts, previously followed at an outside hematology clinic. Despite an extensive workup, no cause for her hyperferritinemia had been identified. She presented to our clinic with new symptoms, including fatigue, exertional dyspnea, hair loss, brittle nails, and pagophagia. Laboratory evaluation revealed anemia with microcytosis—new findings for her—but, notably, her ferritin level remained markedly elevated at over 2,000 ng/mL. The clinical picture raised suspicion for Hereditary Hyperferritinemia-Cataract Syndrome (HHCS), a congenital condition caused by mutations in the 5′ untranslated region of the ferritin light chain (FTL) gene (shown below). This mutation disrupts the normal binding of iron regulatory proteins (IRPs), leading to unchecked ferritin synthesis regardless of iron stores. Indeed, DNA sequencing confirmed a c.-160A>G (Paris-1) mutation that affects apical loop (refers to a specific six-nucleotide sequence at the top (apex) of the iron-responsive element (IRE) hairpin structure found in the 5′ untranslated region (UTR) of the ferritin gene). Given her clinical signs of iron deficiency and the known pathophysiology of HHCS, where elevated ferritin does not reflect iron overload, we initiated treatment for iron deficiency anemia. She experienced a robust improvement in symptoms and Hb following iron repletion.
For larger image, click here.
{kind=link}
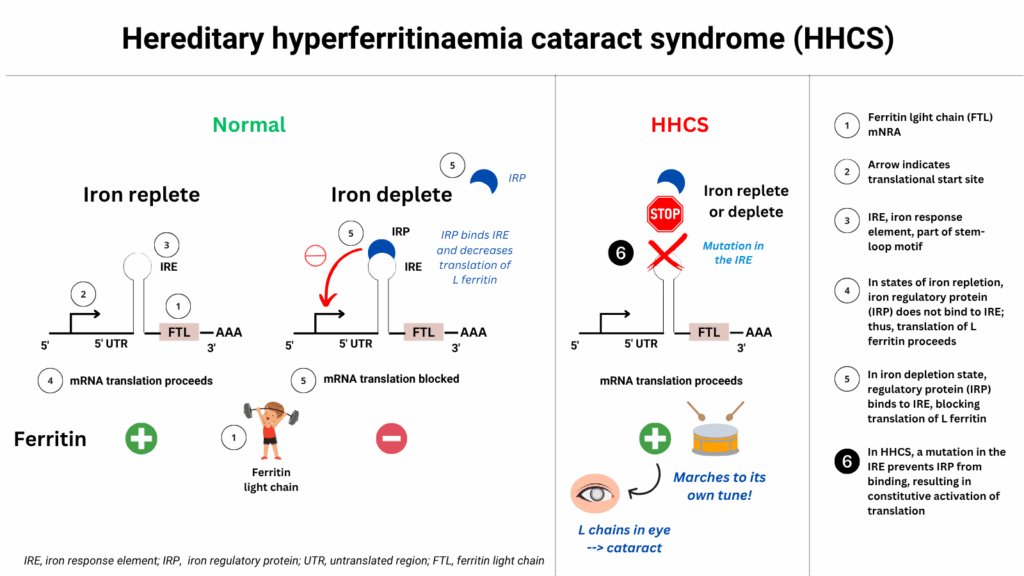
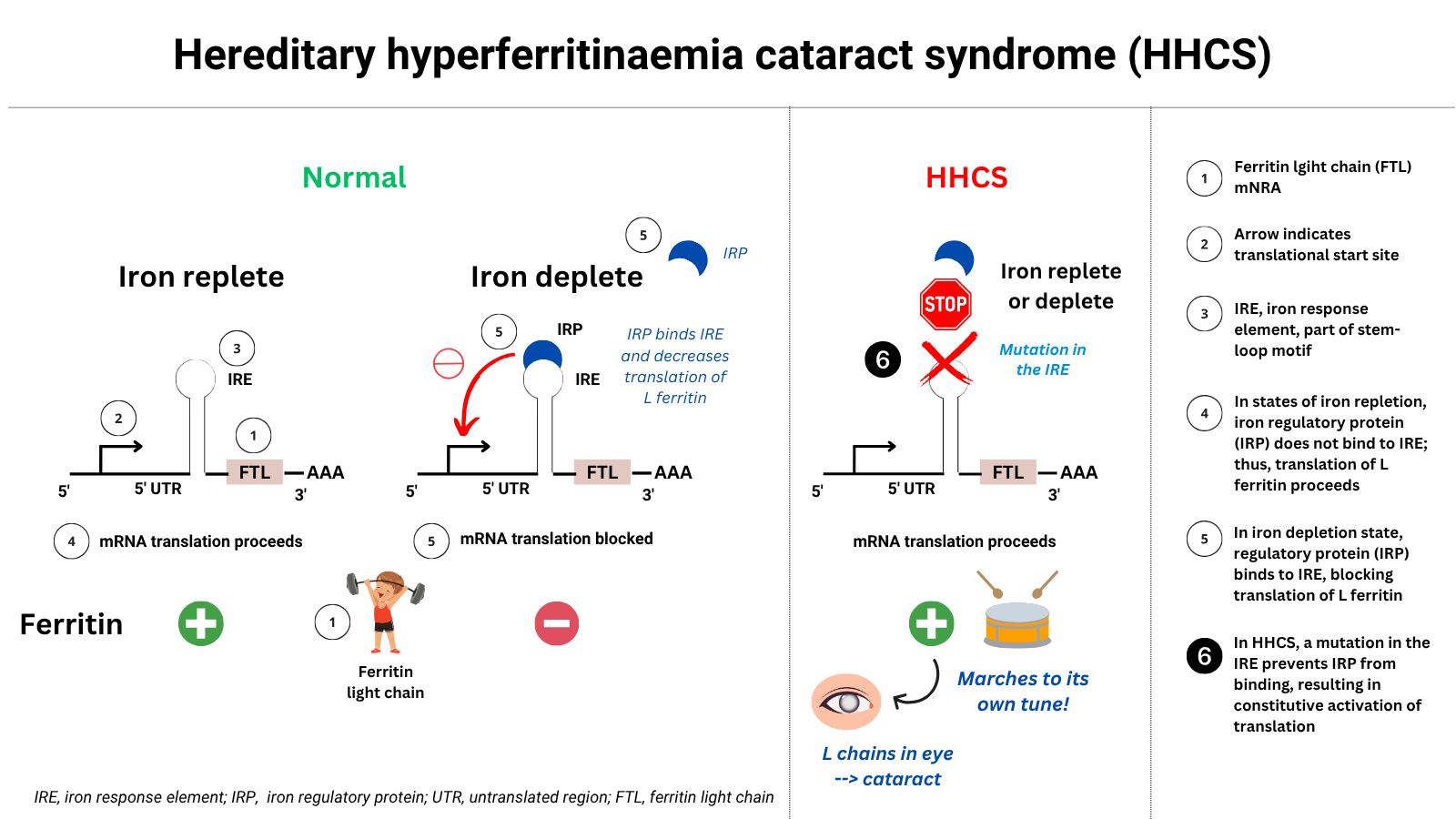
Hereditary Hyperferritinemia-Cataract Syndrome (HHCS):
- Description:
- A rare autosomal dominant disorder characterized by persistently elevated serum ferritin levels from birth, without evidence of iron overload, and the development of bilateral congenital or early-onset cataracts
- Cause:
- Mutation in the iron-responsive element (IRE) of the 5′ untranslated region of the ferritin light chain (FTL) gene
- This disrupts normal post-transcriptional regulation by iron regulatory proteins (IRPs), leading to unchecked ferritin production (unregulated overproduction of L-ferritin) regardless of iron status, even when iron levels are normal
- Over 47 FTL gene mutations have been reported
For larger image, click here.
{kind=link}
- Inheritance:
- Autosomal dominant
- Pathophysiology:
- This excess ferritin circulates in the serum and is also overproduced in tissues, including the lens of the eye
- Ferritin aggregates in the lens fibers form light-scattering crystalline deposits
- These deposits interfere with lens transparency → resulting in bilateral, early-onset cataracts (often in childhood or adolescence)
- Diagnosis:1
- Elevated serum ferritin (often >1000 ng/mL) with normal TSAT and no signs of iron overload
- Pediatric or congenital cataract (breadcrumb-like opacities, scattered white flecks in cortex/nucleus)
- Family history of early cataracts
- Confirmed with genetic testing for FTL IRE mutation
- Management:
- No iron-lowering therapy is needed (e.g., no phlebotomy or chelation)
- Ophthalmologic care: surgical removal of cataracts if vision is impaired
- Important to avoid misdiagnosis as hemochromatosis to prevent unnecessary phlebotomy
| Overview | Rare autosomal dominant disorder characterized by: ✅ High serum ferritin ✅ Bilateral congenital cataracts ✅ No iron overload |
| Biochemical Features | ✅ Ferritin: markedly elevated (often >900–1000 ng/mL) ✅ Transferrin saturation (TSAT): normal ✅ Serum iron: normal ✅ Liver iron: normal (MRI or biopsy) |
| Genetic Basis | ✅ Mutation in iron-responsive element (IRE) of 5′ UTR of the FTL gene (Ferritin Light Chain) ✅ Affects IRP-IRE binding → loss of translational repression → excess L-ferritin production |
| Common Mutations | ✅ c.-160A>G (Paris-1) – affects apical loop ✅ c.-167C>T (Madrid/Philadelphia) – affects C-bulge |
| Pathophysiology | ✅ Excess L-ferritin aggregates in lens fibers ✅ Forms iron-poor crystalline deposits → light scattering → cataracts ✅ Cataracts are bilateral, may be congenital or present in childhood |
| Ophthalmologic Clues | ✅ Breadcrumb-like opacities, scattered white flecks in cortex/nucleus ✅ May be asymptomatic early ✅ Cataracts often precede hyperferritinemia detection |
| Key Diagnostic Clues | ✅ Isolated hyperferritinemia + normal TSAT ✅ Early cataracts in patient or family members ✅ No signs of iron overload despite high ferritin ✅ Family history suggestive of autosomal dominant inheritance |
| Diagnosis | ✅ Serum ferritin + TSAT ✅ Ophthalmology exam (cataract morphology) ✅ Genetic testing: targeted sequencing of FTL IRE region |
| What Not to Do | ✅ Avoid phlebotomy → can cause iron deficiency ✅ Do not misdiagnose as hereditary hemochromatosis |
| Management | ✅ No treatment for hyperferritinemia ✅ Monitor vision, refer for cataract surgery when symptomatic ✅ Genetic counseling for family members |