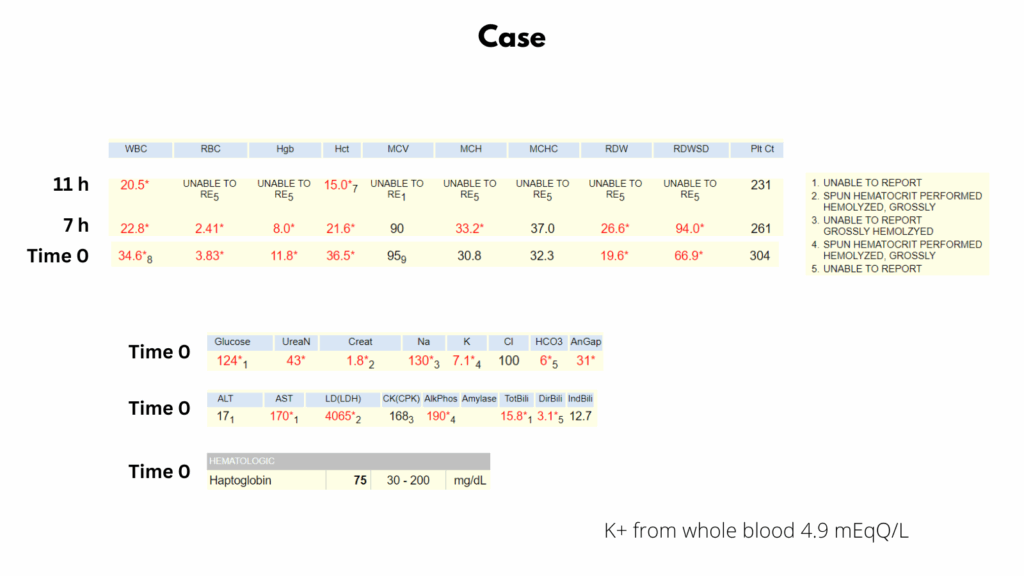
This case involves a 66-year-old man who presented to the emergency department with hypotension and tachycardia. Over the course of just 7 hours, his hemoglobin dropped precipitously from 11.8 to 8.0 g/dL, and by 11 hours it was unmeasurable due to gross hemolysis. Hematocrit measured by microcentrifuge was 15%. Lab studies revealed markedly elevated LDH, AST, and indirect bilirubin, all consistent with intravascular hemolysis. Notably, haptoglobin remained normal, a finding that may seem contradictory but is characteristic of Clostridial sepsis, where impaired clearance of the haptoglobin–hemoglobin complex leads to falsely normal results. Elevated serum (but not whole blood) potassium further supports extensive in vitro hemolysis. This is a classic example of fulminant Clostridium perfringens sepsis, a hematologic emergency requiring urgent recognition and intervention.
Overview
Clostridial sepsis is a rapidly progressive, life-threatening infection caused by bacteria of the genus Clostridium, most commonly Clostridium perfringens. This rare but devastating form of sepsis often affects people with underlying conditions such as gastrointestinal or genitourinary disease, malignancy, immunosuppression, or after surgical or traumatic tissue injury. It is a medical emergency that requires prompt recognition and aggressive treatment due to its fulminant course, potential for massive intravascular hemolysis, and high mortality.
Key features of Clostridial sepsis:
| Aspect | Details |
|---|---|
| Causative agents | Clostridium perfringens (most common), C. septicum, C. sordellii, etc. |
| Type of bacteria | Gram-positive, anaerobic, spore-forming rods |
| Source of infection | GI or genitourinary tract, infected wounds, or post-surgical sites |
| Risk factors | Immunosuppression, diabetes, trauma, malignancy (esp. GI tumors), recent surgery, necrotic tissue |
Pathogenesis:
- Clostridial species are anaerobic, spore-forming, Gram-positive bacilli found in soil and in the human gut.
- Infection may follow tissue trauma, gut perforation, gynecologic procedures, or occur in immunosuppressed patients or those with cancer.
- The bacteria produce potent exotoxins (notably alpha-toxin from C. perfringens) that cause rapid tissue destruction, hemolysis, and shock.
- Clostridium perfringens alpha toxin is responsible for gas gangrene and myonecrosis in infected tissues. The toxin also possesses hemolytic activity.

Crystal structure of Clostridium perfringens alpha toxin; from Wiki
Clinical presentation:
- Sudden onset of fever, chills, hypotension, and shock
- Severe hemolysis (hallmark of C. perfringens sepsis):
- Rapid drop in hemoglobin
- Dark or black-colored plasma (due to free hemoglobin)
- Elevated LDH, indirect hyperbilirubinemia
- Normal or falsely elevated haptoglobin (due to assay limitations)
- Spherocytes and ghost cells on blood smear
- Leukemoid reaction or profound leukocytosis
- Multi-organ failure
- Gas formation in soft tissues or bloodstream (may be seen on imaging or blood cultures)
- May also present with myonecrosis or gas gangrene (in limb or surgical site)
Hematologic manifestations:
- Acute massive intravascular hemolysis
- Up to 15% of patients with C. perfringens sepsis experience acute massive intravascular hemolysis, causing rapid anemia, spherocytosis, hemoglobinemia, hemoglobinuria, and jaundice.
- Blood and serum can appear bright red due to free hemoglobin
- Due to the action of potent clostridial exotoxins, particularly alpha toxin
- Leukemoid reaction
- Thrombocytopenia
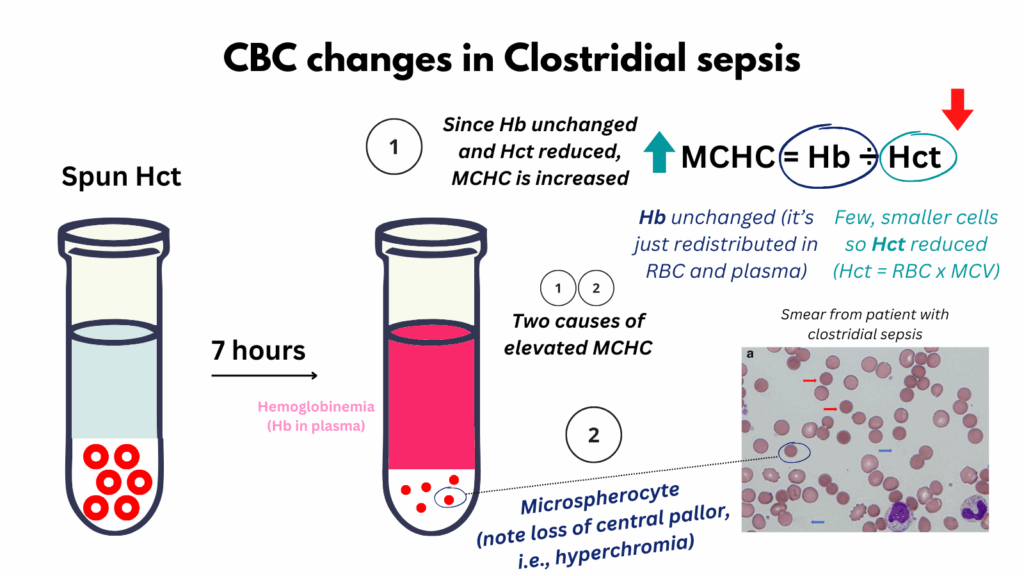
This graphic illustrates key changes in the complete blood count (CBC) observed in Clostridial sepsis, a condition characterized by massive intravascular hemolysis. First, hemolysis releases large amounts of hemoglobin into the plasma. Standard hemoglobin assays measure total hemoglobin regardless of its location, intracellular or free in plasma, so the measured hemoglobin concentration may remain unchanged, even as red cell mass declines. In contrast, the spun hematocrit, which reflects the fractional red cell volume, reveals a true loss of red cell mass. As a result, the mean corpuscular hemoglobin concentration (MCHC), calculated as hemoglobin divided by hematocrit, appears falsely elevated. However, there is also a true elevation in MCHC due to morphologic changes in surviving red blood cells. These become smaller and more spherical, forming microspherocytes with loss of central pallor (sometimes called hyperchromic microsites). This shape change increases the relative concentration of hemoglobin within individual red cells, contributing to the elevated MCHC in a physiologically meaningful way. Finally, the reduced red cell size (decreased MCV) contributes further to the fall in hematocrit, since hematocrit = MCV × RBC count.
Diagnostic clues:
- Gram stain: Large gram-positive rods with few or no inflammatory cells
- Blood cultures: Often positive within hours; Clostridium species grow rapidly
- Imaging: May show gas in soft tissues or organs
- Labs:
- Hemolysis panel: ↓Hb, ↑LDH, ↑indirect bilirubin, low/false normal haptoglobin
- Marked discrepancy between red blood cell count and hemoglobin
- Elevated creatinine and liver enzymes from shock and hemolysis
- Elevated white cell count with left shift
- Thrombocytopenia
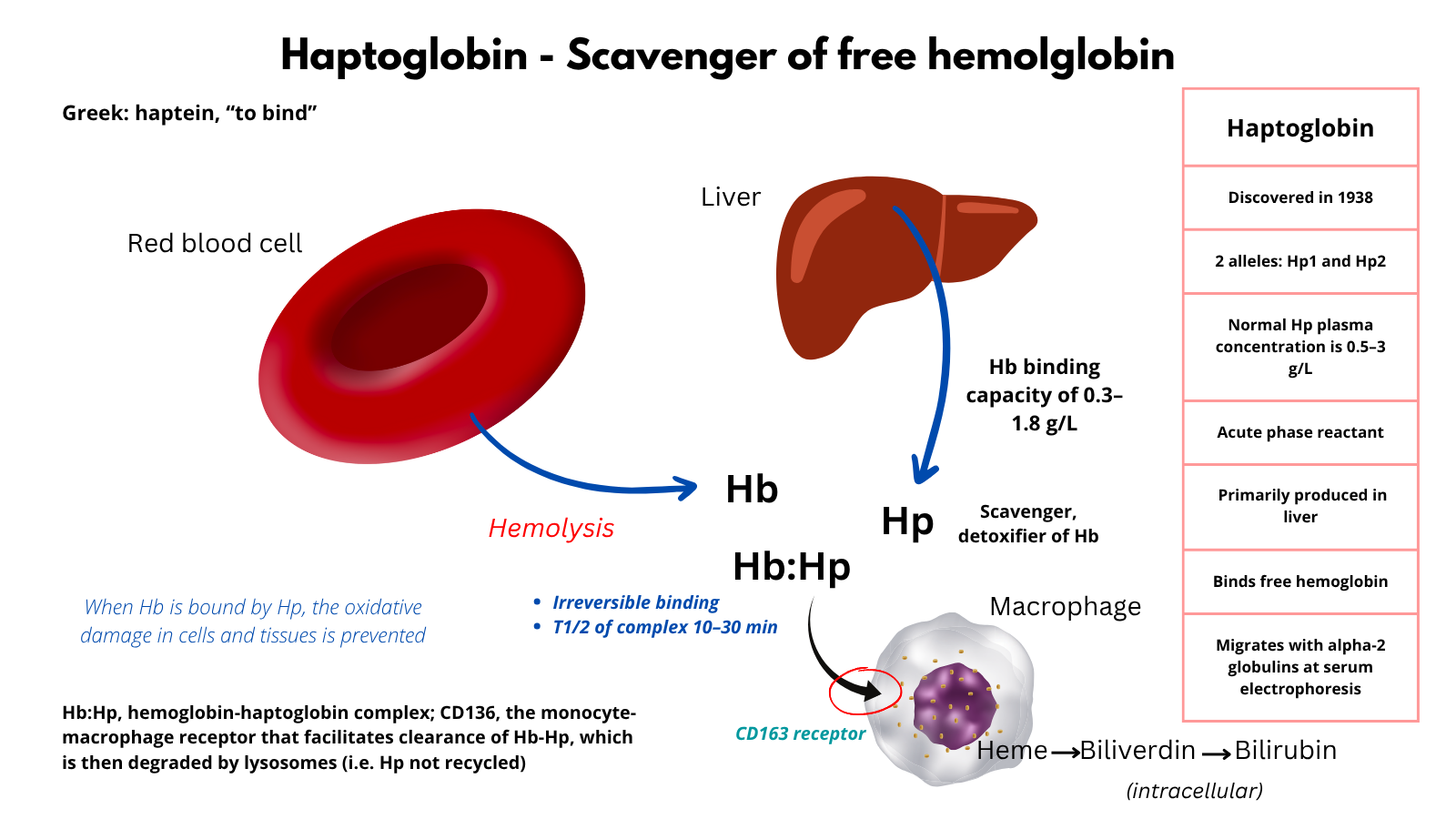
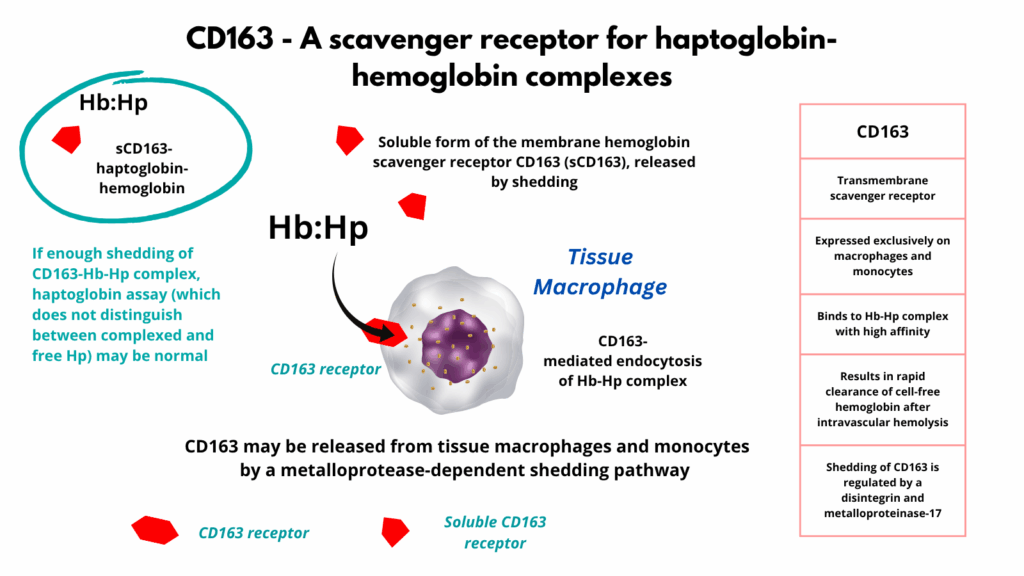
Note: in Clostridial sepsis, the haptoglobin may paradoxically appear normal or falsely elevated because the essay does not differentiate free haptoglobin from haptoglobin hemoglobin complexes. This occurs because there is interference with receptor mediated clearance of the haptoglobin hemoglobin complex by the alpha toxin. Specifically, uptake of the complex by CD163 receptors on macrophages may be disrupted (or shed), leading to the accumulation of the complex in the plasma. This results in preserved or even elevated measure haptoglobin levels despite ongoing hemolysis. A normal haptoglobin in a patient with signs of massive intravascular hemolysis (especially with dark plasma and gram-positive rods in blood) should immediately raise suspicion for Clostridial sepsis.

For larger image, click here.
{kind=link}
For larger image, click here.
{kind=link}
Treatment:
- Antibiotics (ASAP)
- High-dose IV penicillin G + clindamycin (inhibits toxin production)
- Surgical intervention
- Debridement of necrotic tissue, drainage of abscess, or amputation if needed
- Hemodynamic support
- Fluids, vasopressors, ICU care
- Transfusion
- Supportive care for hemolysis and anemia
- Hyperbaric oxygen therapy
- Sometimes used in gas gangrene, though evidence is limited
Prognosis:
- Very high mortality; up to 70–100% in cases with massive hemolysis or delayed treatment
- Death may occur within hours if not recognized and treated aggressively
Takeaways:
- Think Clostridial sepsis in a patient with rapid-onset shock, massive hemolysis, and gram-positive rods on blood smear or cultures.
- The presence of dark plasma, hemolysis with falsely normal haptoglobin, and gas in tissues is highly suspicious.
- Treatment must be immediate and aggressive, with antibiotics, surgery, and ICU-level support.
Back to the patient

For larger image, click here.
{kind=link}