Ferritin – Case Studies

A reminder about upper limit of normal range for serum ferritin. According to British Society of Haematology:

Repeat iron indices demonstrate a similarly elevated ferritin and TSAT.

The patient is otherwise well, has not received transfusions and denies alcohol intake. You order a CRP and liver function tests, which are normal.
According to British Society of Haematology:
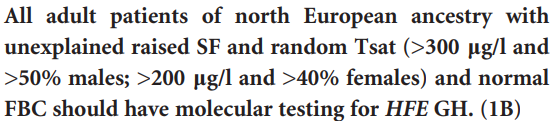
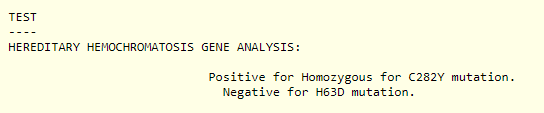
The results for the hereditary hemochromatosis screen are the following:
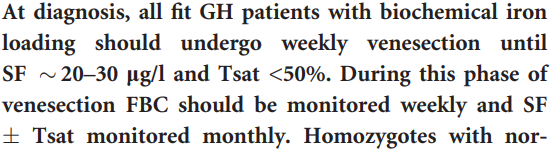
According to British Society of Haematology:


According to the ACG Clinical Guideline:
Treatment should be initiated in C282Y homozygotes with an elevated SF, defined as >300 ng/mL in men and >200 ng/mL in women, along with a TS of >45%.. Although patients with a SF of >1,000 ng/mL at the time of diagnosis are unlikely to have end-organ damage from HH, we still suggest treatment in this population considering that between 13% and 35% of men and between 16% and 22% of women will progress to a SF of >1,000 ng/mL if left untreated.
Am J Gastroenterol. 2019 Aug;114(8):1202-1218

According to British Society of Haematology Guideline:

What are the most likely explanations for this set of lab results (choose two)?
Here are some additional labs:


Which of the following statement(s) is/are true (more than one answer may apply):
Ferritin is an acute phase reactant.
