Quiz 1 – Red Cell Indices
By William Aird
Abbreviations:
Hb – hemoglobin
Hct – hematocrit
MCH – mean corpuscular hemoglobin
MCHC – mean corpuscular hemoglobin concentration
MCV – mean cell colume
RBC – red blood cell count
RDW – red blood cell distribution width
RDW-CV – RDW coefficient of variation
RDW-SD – RDW standard deviation
Note: The terms MCV, MCH and MCHC are all mean values and by definition apply to populations of red cells. To simplify matters, we use the term more loosely to include descriptions of single cells. For example, we may refer to a large red cell as one with a high MCV, or a cell with increased central pallor as one with a low MCHC.

Spun hematocrits
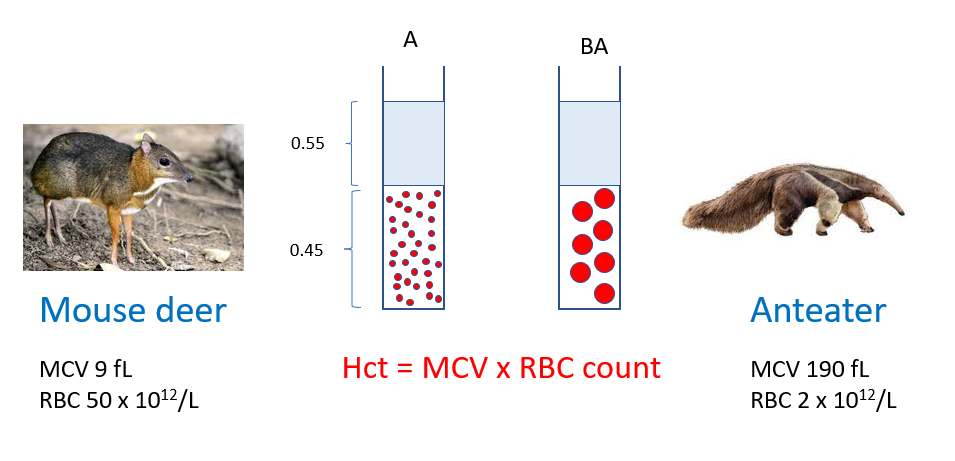
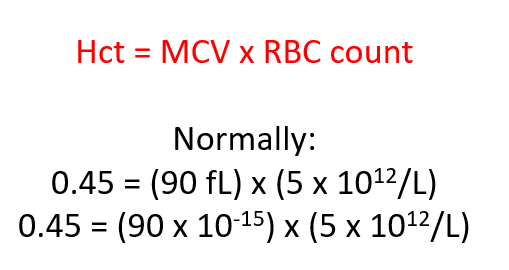
Remember:
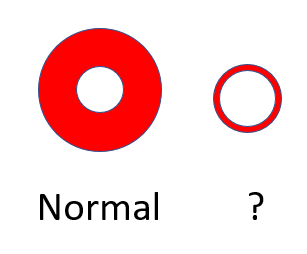
Question 8
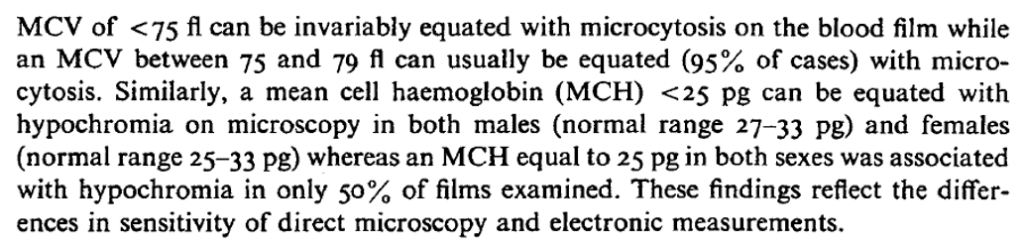
How would you describe the red cell on the right (schematic of a normal red cell is shown on the left)?
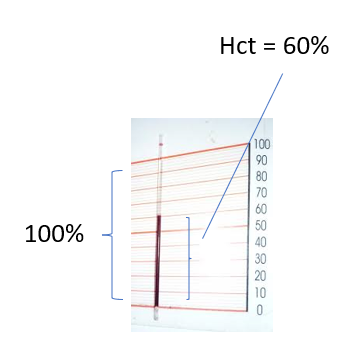
Spun Hct




Question 10
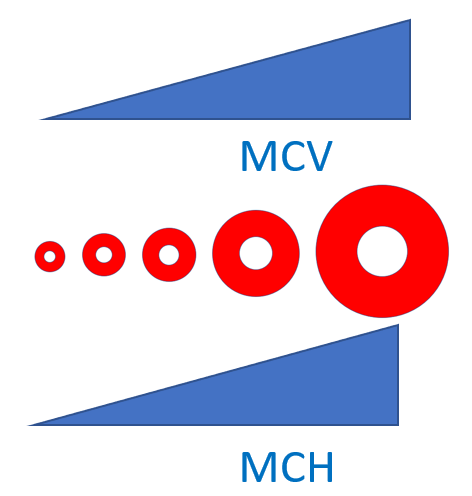
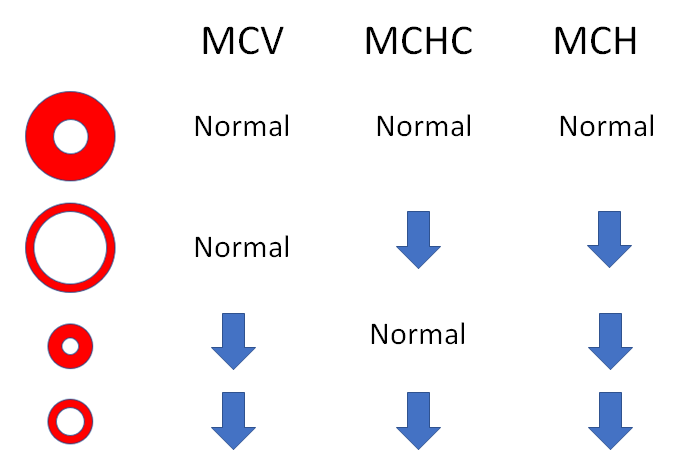
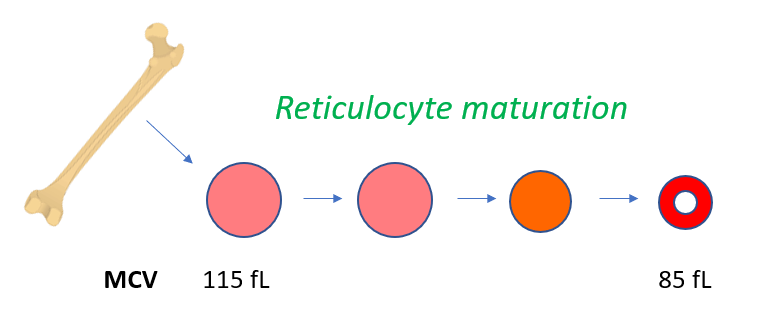
What is happening to the mean cell hemoglobin (MCH) moving left to right (assume a constant central pallor or MCHC)?
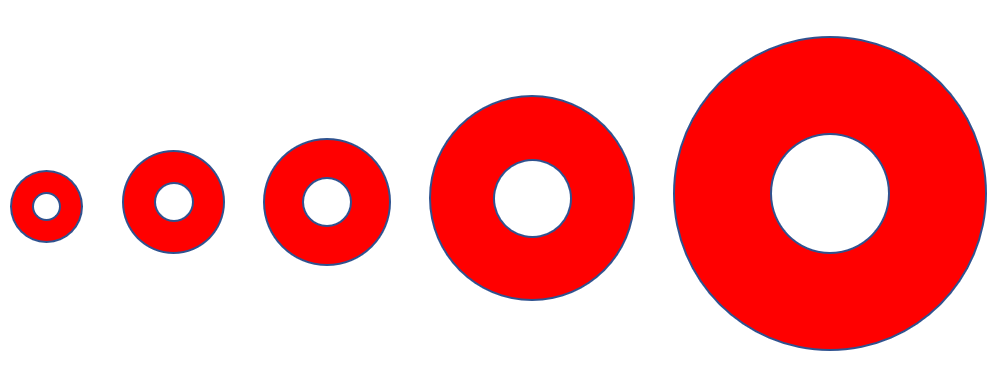
Question 10
MCH tracks with the MCV
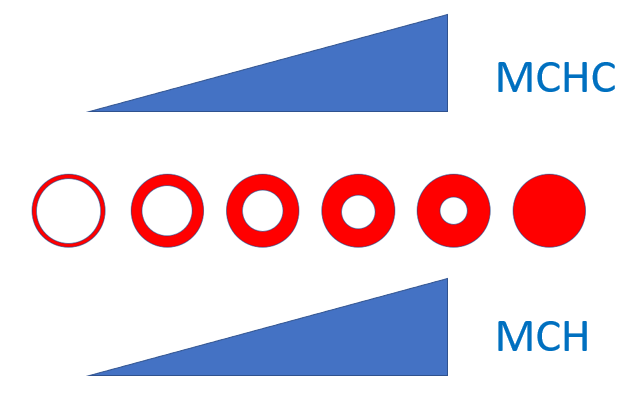
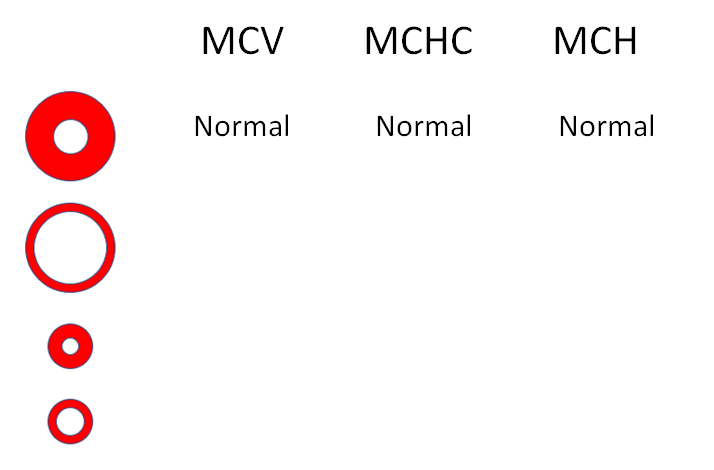
Question 11
What is happening to the mean cell hemoglobin (MCH) in this series of red cells (moving left to right)? Note that the red cell volume is the same in all cells.

Question 11
MCH also tracks with the MCHC
Question 12 (cont’d)
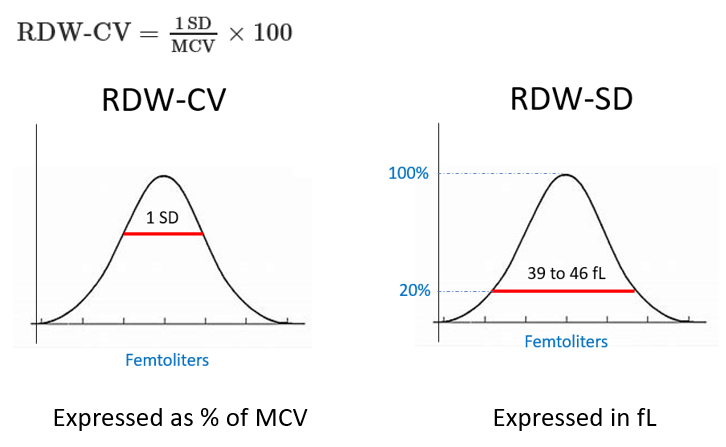
The RDW-CV measures size dispersion by means of a ratio formula of 1 standard deviation to the MCV, and is expressed as a percentage of the MCV (reference range of 11% to 16%)
The RDW-SD is the arithmetic width of the distribution curve measured at the 20% frequency level and is expressed as standard deviation in femtoliters (fL) (reference range 39-46 fL)
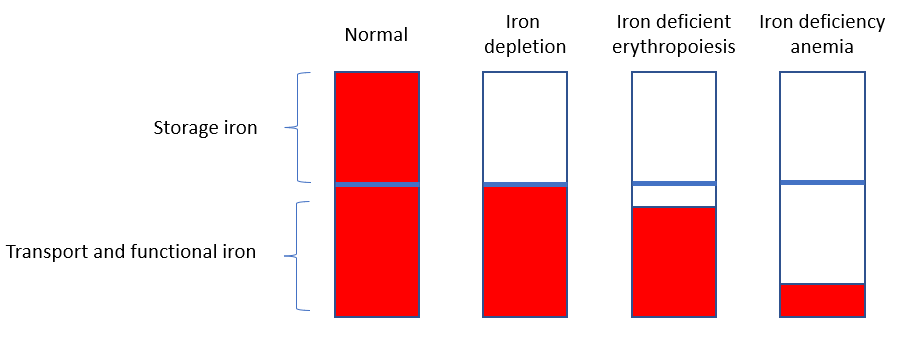
Stage 1 – iron depletion
- Storage iron depleted (primarily macrophages)
- Only remaining iron is in the transport and functional (e.g. Hb) pools
- Serum ferritin (marker of iron stores) low
Stage 2 – Iron deficient erythropoiesis
- Reduction of transport iron
- Decreased serum iron
- Increased total iron binding capacity (TIBC) to maximize iron transport to red cells
- Increased expression of transferrin receptor on RBC membrane to promote iron uptake
Stage 3 – Iron deficiency anemia
- RBCs are no longer able to compensate, and production falls
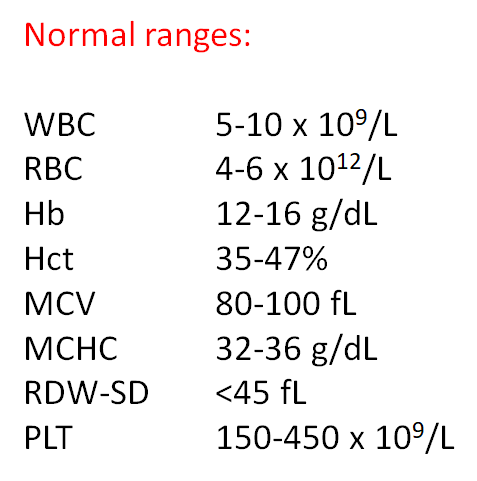
Question 17
Describe the CBC (answer on next slide)
| WBC | Hb | Hct | MCV | MCHC | RDW-SD | PLT |
|---|---|---|---|---|---|---|
| 5.6 | 17.8 | 54 | 70 | 33 | 52 | 440 |
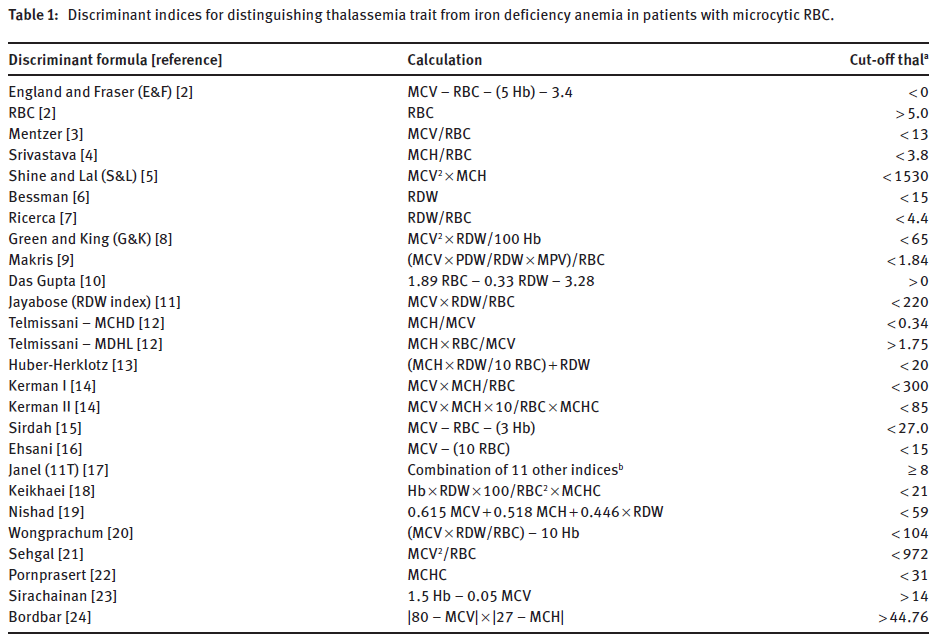
Discriminatory formulas for distinguishing thalassemia from iron deficiency in patients with microcytic anemia (the Mentzer index is third from the top)
Question 23
Fill in the parameters: Normal, increased or decreased (answer on next page)
Question 23 (cont’d)
Fill in the parameters: Normal, increased or decreased (answer on next page)
Question 29
What is wrong with the following statement (answer on next slide)?
Question 31
Which RBC best describes the phenotype in hypernatremia when measured in vitro (as part of a CBC)?
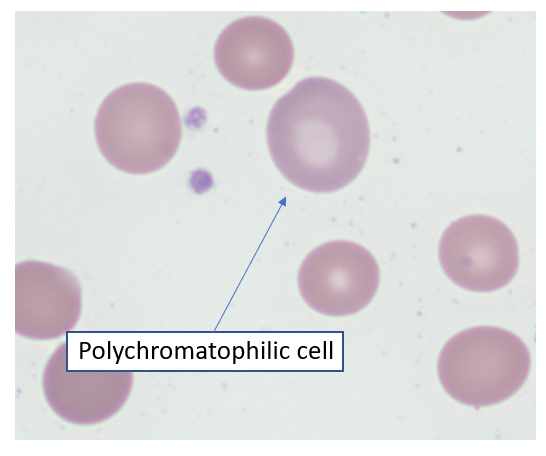
Wright Giemsa stain showing polychromatophilic cell. According to the College of American Pathologists, polychromatophilic cells are nonnucleated, round, or ovoid red cells staining homogeneously pink-gray or pale purple. They are larger than mature RBCs and usually lack central pallor
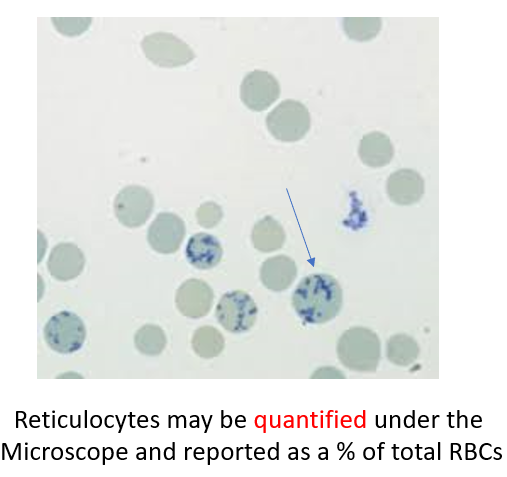
On supravital stains (meaning that the slide is stained without prior fixation – the RBCs are still “alive” when they are incubated with the staining solution), reticulocytes are identified by clumped granular material called reticulum (this is where the term “reticulocyte” comes from). Reticulum consists of aggregates of residual ribosomes mitochondria.
values from increased production and shortening of marrow maturation time (leading to increased retic circulation time).