Quiz – Platelets high and low
By William Aird
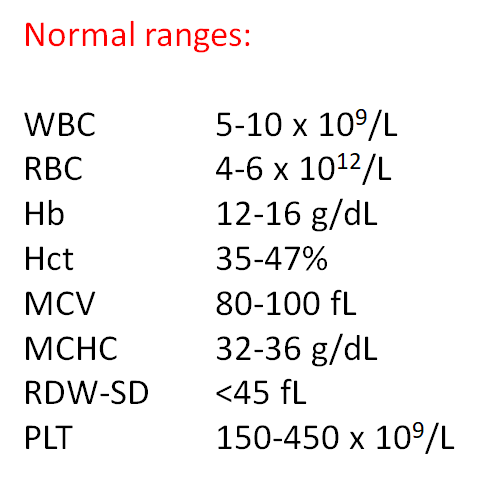
Abbreviations:
Hb – hemoglobin
Hct – hematocrit
MCH – mean corpuscular hemoglobin
MCHC – mean corpuscular hemoglobin concentration
MCV – mean cell colume
RBC – red blood cell count
RDW – red blood cell distribution width
RDW-CV – RDW coefficient of variation
RDW-SD – RDW standard deviation
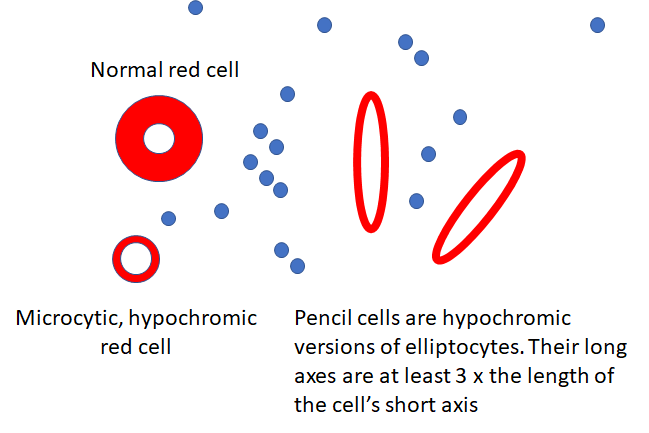
Note: The terms MCV, MCH and MCHC are all mean values and by definition apply to populations of red cells. To simplify matters, we use the term more loosely to include descriptions of single cells. For example, we may refer to a large red cell as one with a high MCV, or a cell with increased central pallor as one with a low MCHC.
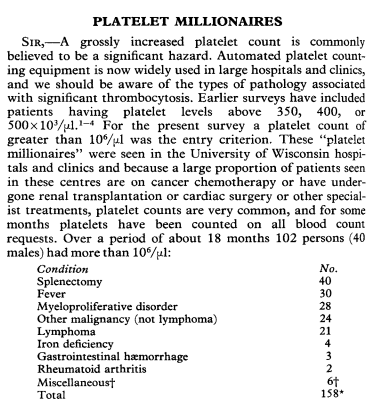
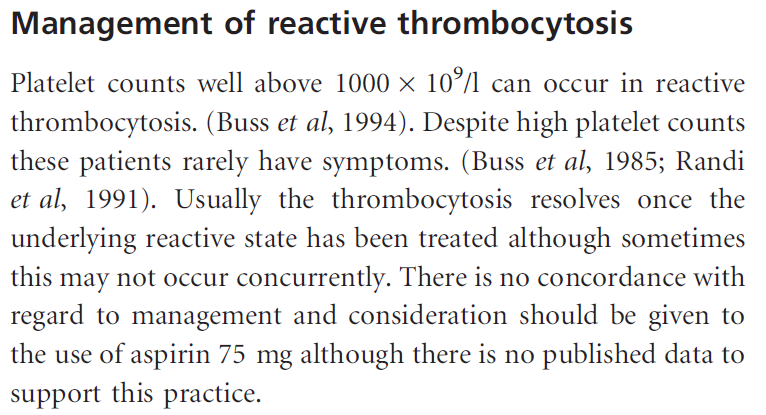
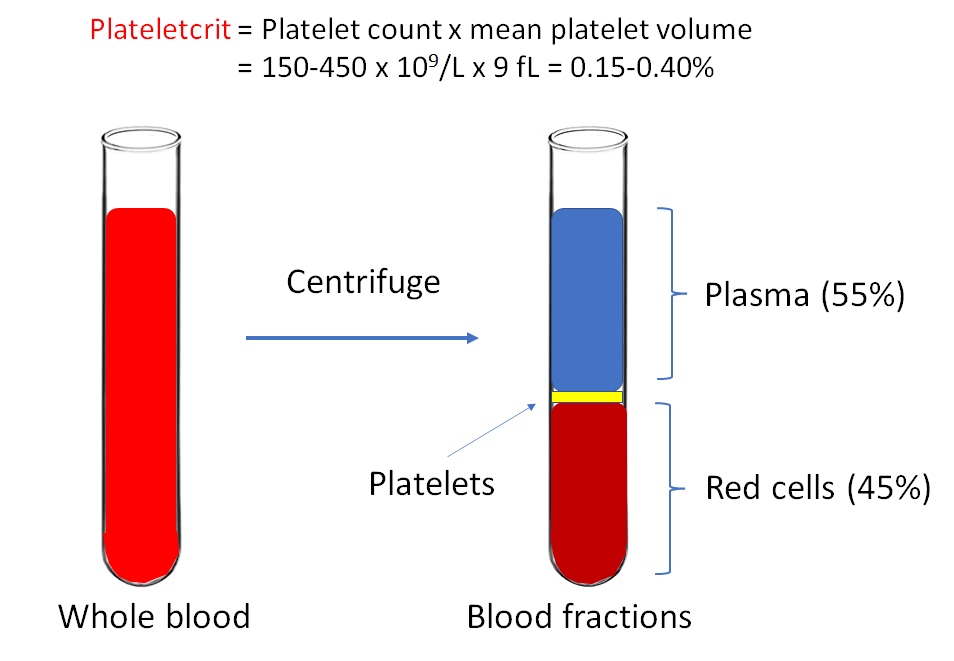
Patients with extreme thrombocytosis have been referred to as platelet millionaires! That is because 1000 x 109/L is 1 million/ul.

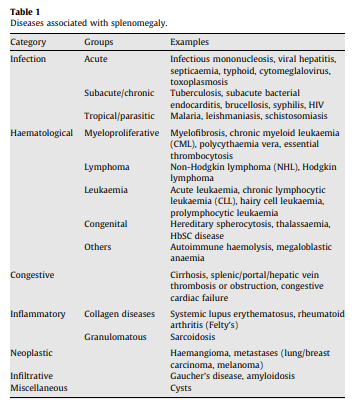
Splenomegaly is more common in myelofibrosis than in essential thrombocythemia or polycythemia vera
A reminder of the differential diagnosis of splenomegaly:

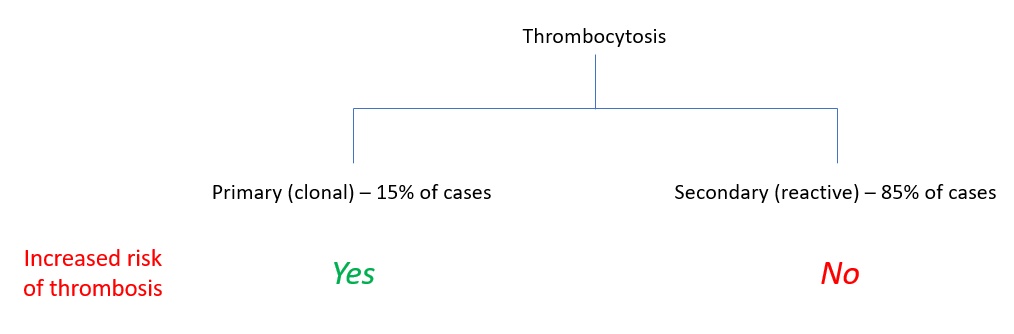
In the interest of full disclosure, the single guideline that is focused on “investigation and management of adults and children presenting with a thrombocytosis” from 2010 suggests considering the use of aspirin in patients with secondary (reactive) thrombocytosis, but it is doubtful that most clinicians would agree with this:
From D. Saintillan:
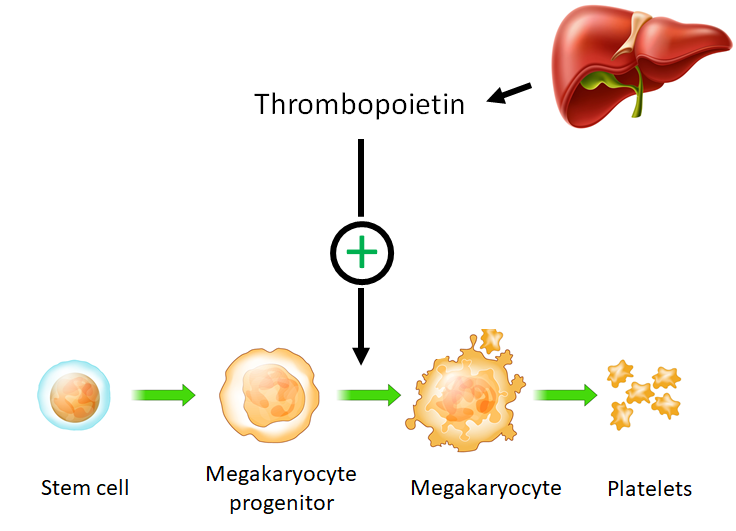
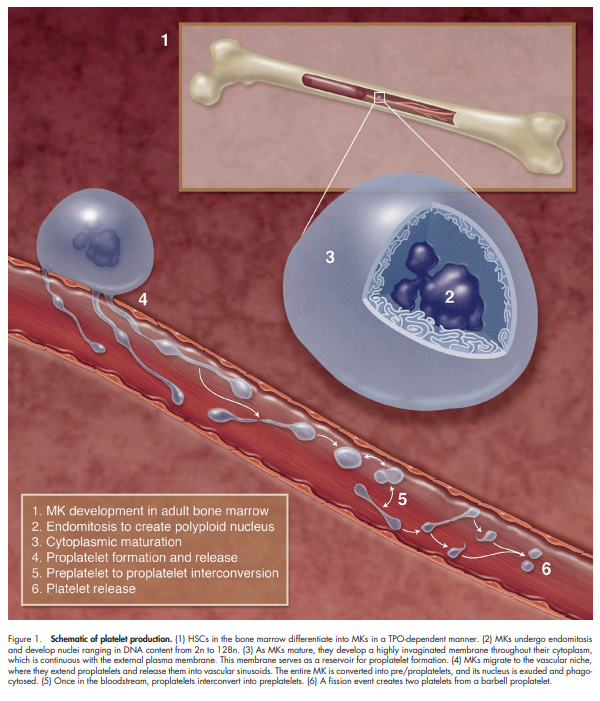
The in vivo production of platelets takes place inside bone marrow, where large cells known as megakaryocytes develop long tubular membrane projections, or proplatelets, which continuously break up into small fragments destined to mature into functional platelets and enter the blood stream. The formation and growth of these tubular structures and their subsequent fragmentation are driven by ATP-powered processes involving biopolymers and molecular motors.
From Machlus and Italiano:
To assemble and release platelets, MKs become polyploid by endomitosis (DNA replication without cell division) and then undergo a maturation process in which the bulk of their cytoplasm is packaged into multiple long processes called proplatelets, and the nucleus is extruded. An MK may extend 10–20 proplatelets, each of which starts as a blunt protrusion that over time elongates, thins, and branches repeatedly. Platelets form selectively at the tips of proplatelets. As platelets develop, they receive their granule and organelle content as streams of individual particles transported from the MK cell body

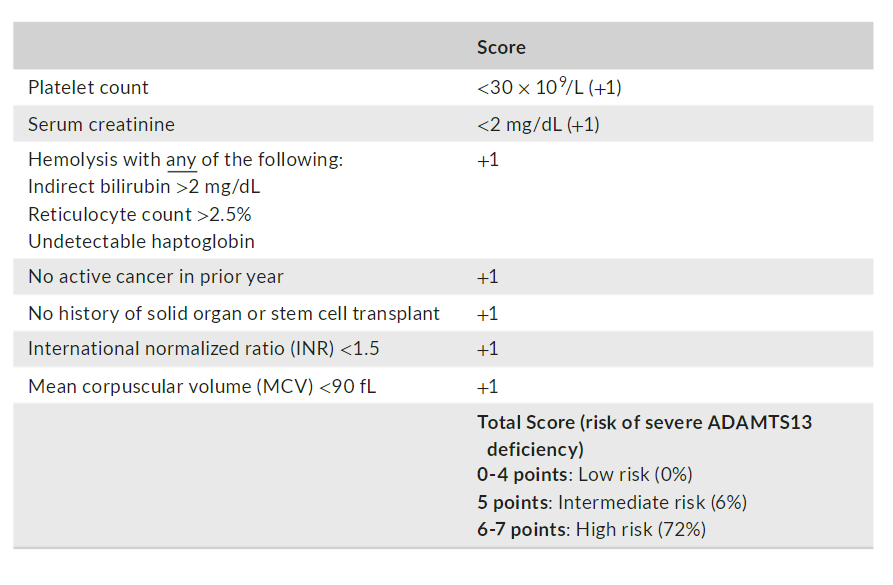
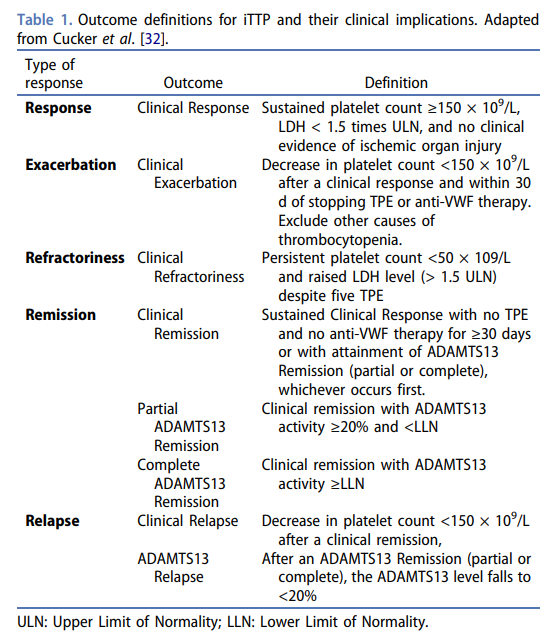
n a recent publication, high scores of 6- 7 versus low/intermediate scores of 0- 5 predicted severe ADAMTS13 deficiency with a positive predictive value of 72%, negative predictive value of 98%, sensitivity of 90%, and specificity of 92%
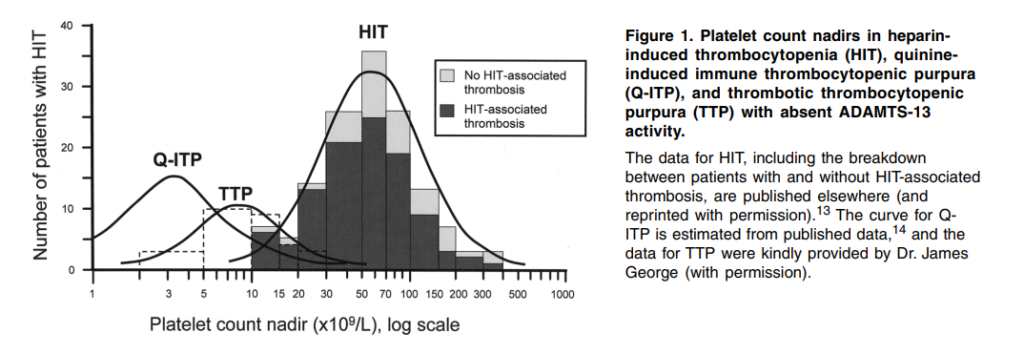
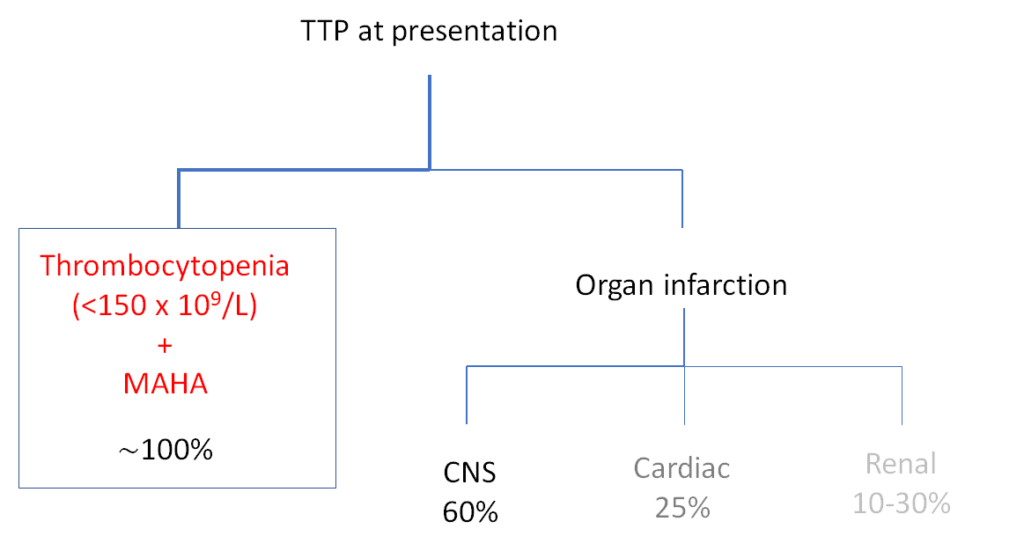
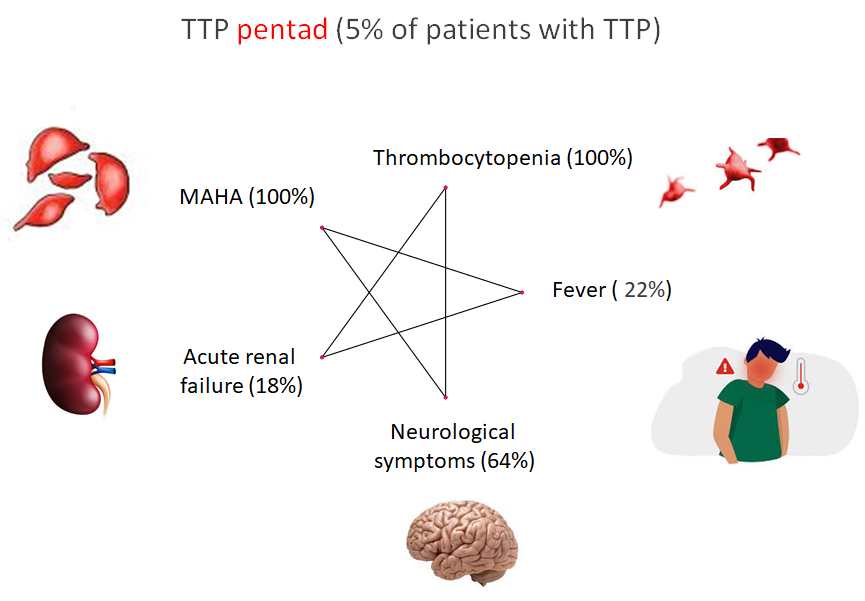
MAHA; microangiopathic hemolytic anemia; prevalence figures from J Clin Apher 2014;29:148