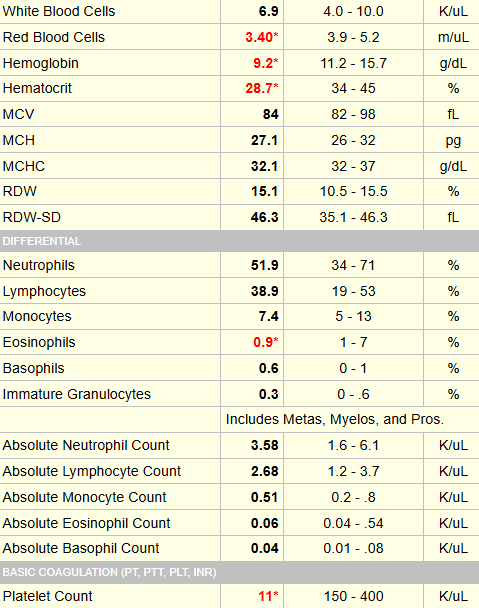
42 yo M with Hemolytic Anemia and Thrombocytopenia
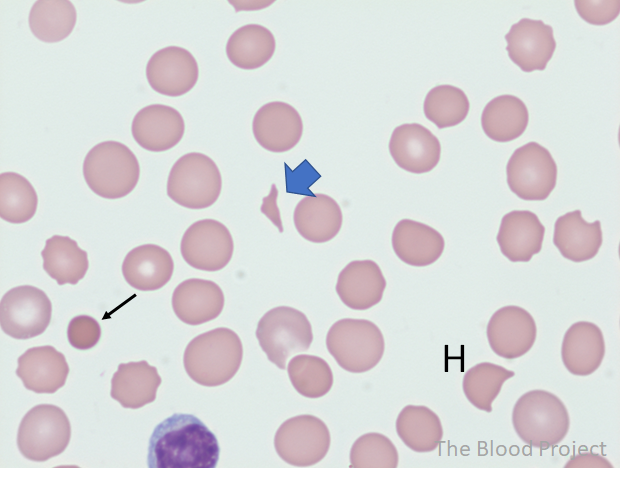
The smear was similar to the one shown below:
So far, the data are most consistent with a diagnosis of TMA. There are many different causes of TMA. One of these, TTP, has a mortality of about 90% if left untreated.
This patient had blood drawn for ADAMTS13 activity level at the time of admission. However, this is a send out test and takes 3-4 days to come back. We cannot afford to wait this long to decide on treatment. Instead, we use a clinical prediction rule to determine pretest probability of having TTP and empirically treat those who are at high risk.
The results of the PLASMIC score in this case are shown below:

In response to corticosteroids and TPE, the patient’s platelet count (and haptoglobin, not shown) increased nicely with normalization after 5 daily therapeutic exchanges (with one volume per exchange):
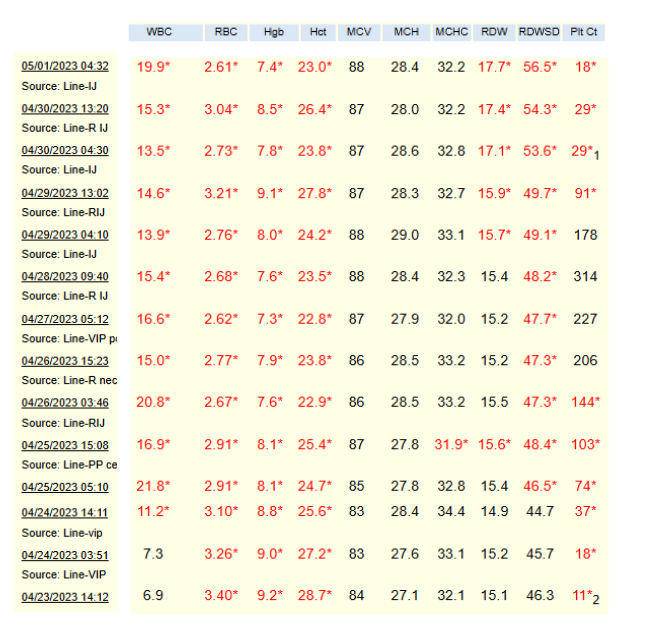
This patient had a clinical response, which is defined as a sustained normalization of platelet count (for example, > 150 × 109/L) and lactate dehydrogenase (LDH) level < 1.5 times the upper limit of normal after cessation of plasma exchange.
However, his platelet count subsequently fell again within several days, requiring reinstitution of therapeutic plasma exchange. This qualifies as an exacerbation, defined as a fall in platelet count to below the lower limit of the reference range (for example, < 150 × 109/L) requiring reinitiation of plasma exchange within 30 days of the last plasma exchange after initial clinical response had been achieved.
As shown in the next slide, he responded well to reinitiation of therapeutic plasma exchange.

The results of the ADAMTS13 activity assay came back 4 days after the patient was admitted:

What statement is correct (choose one):
The patient had an ADAMTS13 inhibitor study done, which was positive, indicating this was a case of immune TTP.

The patient did well and was discharged in remission. He received one additional treatment, which continued as an outpatient.