IV Iron
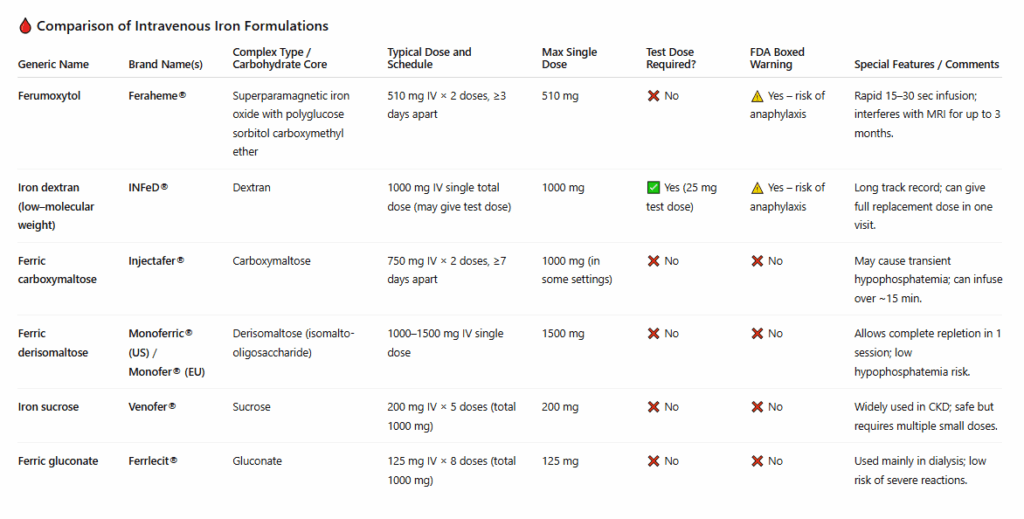
- Feraheme® (ferumoxytol) and INFeD® (iron dextran) both carry boxed warnings for rare anaphylaxis.
- Ferric carboxymaltose and ferric derisomaltose allow large single doses, improving convenience.
- Iron sucrose and ferric gluconate are older, well-studied, and very safe but require multiple infusions.
- Ferric carboxymaltose commonly causes hypophosphatemia, whereas derisomaltose does not.
- Ferumoxytol is unique in being MRI-interfering and rapidly infused.

Match the generic with the brand name
Ferumoxytol
Low-molecular-weight iron dextran
Iron sucrose
Infed
Feraheme
Venofer
Correct!
Sorry, Incorrect.
Match the generic with the brand name
Ferric gluconate
Ferric derisomaltose
Ferric carboxymaltose
Ferrlecit
Injectafer
Monoferric
Correct!
Sorry, Incorrect.
Match the IV iron formulation (Column A) to the key feature (Column B)
Iron sucrose
Iron dextran
Ferumoxytol
Typically 5 clinic visits to deliver ~1 g
The only prep that uses a test dose
2 clinic visits to deliver a full course (510 mg × 2).
Correct!
Sorry, Incorrect.
Match the IV iron formulation (Column A) to the key feature (Column B)
Ferric gluconate
Ferric carboxymaltose
Ferric derisomaltose
Single visit total-dose infusion
Hypophosphatemia risk signal.
Often multiple visits (≈8) t
Correct!
Sorry, Incorrect.

Match the clinical scenario (Column A) with the appropriate indication (Column B).
Pregnant woman who vomits with every oral iron dose
Menstrual blood loss causing mild anemia, patient tolerating oral iron
Patient with Crohn’s disease and iron deficiency anemia not responding to oral iron
Intolerance or non-adherence to oral iron
Malabsorption or inflammatory bowel disease
Oral iron adequate—no indication for IV iron
Correct!
Sorry, Incorrect.
Sort the following clinical scenarios into the correct category:
Mild iron deficiency responding to oral iron
Post–gastric bypass with malabsorption
Heart failure with iron deficiency
Athlete with low ferritin but normal Hb
IBD with intolerance to oral iron
Preoperative anemia, imminent surgery
Iron deficiency without anemia (unless special circumstances)
Celiac disease with poor absorption
CKD on ESA therapy
Pregnant patient intolerant to oral iron
IV Iron Indicated
IV Iron Not Indicated