Knowledge Check

Sort the causes of elevated activated partial thromboplastin time (top) according to whether or not they are associated with an increased risk of bleeding (bottom):
Factor XII deficiency
Factor VIII deficiency
Factor IX deficiency
Lupus anticoagulant
Factor XI deficiency
No bleeding risk
Bleeding risk

Contact pathway. Factor XII (FXII) is activated by negatively charged surfaces. FXIIa activates factor XI (FXI) (not shown) and plasma prekallikrein (PK) to FXIa and kallikrein, respectively. In a positive feedback loop, kallikrein hydrolyzes FXII, amplifying FXIIa formation. Kallikrein also releases the proinflammatory mediator bradykinin from high molecular weight kininogen (HK). Both PPK and FXI circulate in plasma bound to HK.
A study in 2019 reported on the systematic evaluation of all causes of aPTT prolongation in a consecutive population of 187 outpatients referred for specialized hemostasis consultation during a 14‐year period. 65.8% had an isolated elevation of the aPTT, though the causes were not stratified according to whether or not the elevation was isolated. The results are shown in the following two figures followed by the authors’ take home messages:
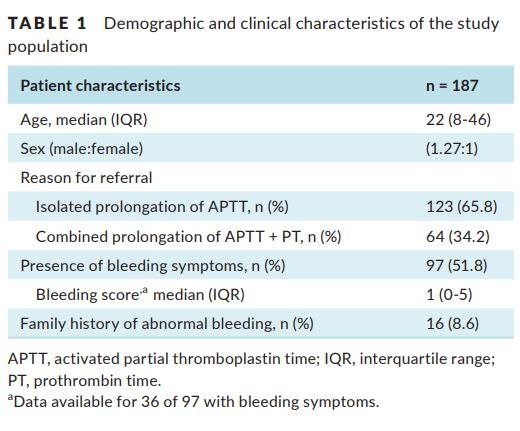
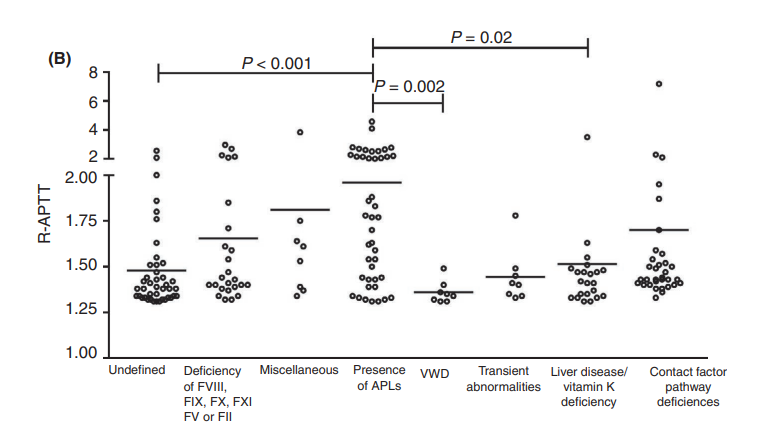
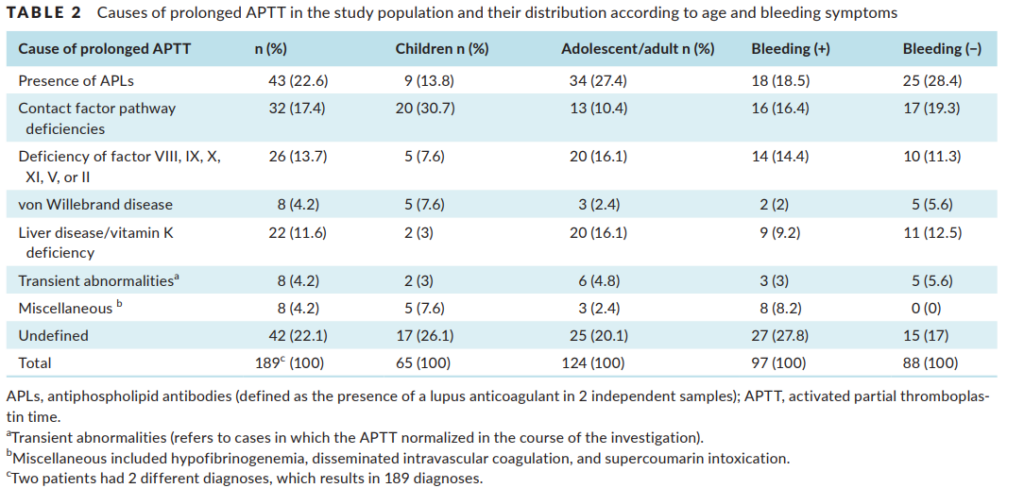
Take home messages:
- Presence of APL (which in this study included all patients with a positive LA in at least 2 independent samples) was the main cause of prolonged aPTT.
- Contact pathway factor deficiencies emerged as the third most frequent cause.
- Definitive explanation for the prolonged aPTT could not be obtained in 22.1% of patients despite a comprehensive investigation.
- Previously undiagnosed liver disease was also an important cause of aPTT prolongation (in nearly 10% of patients).
- Normalization of the aPTT still occurred in almost 5% of cases, highlighting the importance of repeating the assay in the course of the investigation.