Case TTP
The answer to these questions was no. The physical exam was unremarkable except for gravid uterus.
Here is the patient’s CBC, WBC differential and reticulocyte count at presentation:

What are two buckets of causes of elevated reticulocyte count in the setting of anemia?
Click for Answer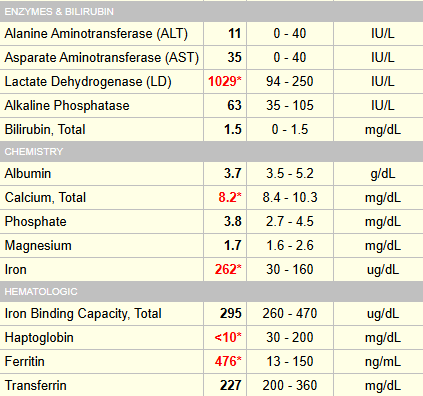
Let’s take a look at the peripheral smear:

What does the smear show?
Let’s look at more lab data at admission:


Renal function and liver function normal, arguing against aHUS or HELLP.
Hematology progress note (day 2):

The patient presented with headache and facial numbness. A CT head was ordered, which was normal:

Maternal fetal medicine (day 1):

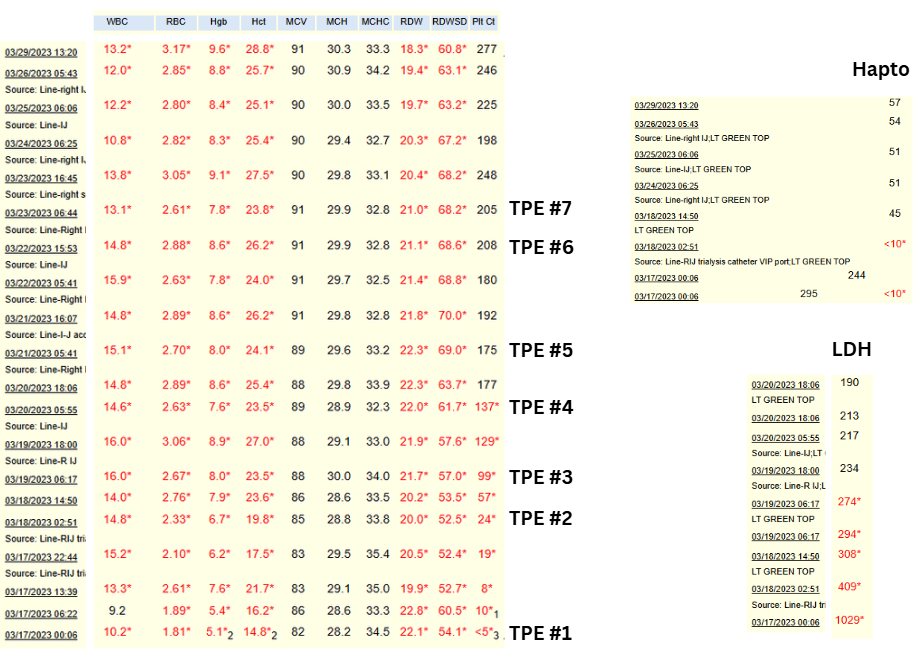
Time series of CBC, haptoglobin and LDH while in hospital:
Results of ADAMTS13 activity level (came back on day 5):

Are these results consistent with a diagnosis of TTP?

The patient was discharged after 9 days (7 sessions of therapeutic plasma exchange) on prednisone 60 mg daily (tapered down to 15 mg at time of delivery), aspirin 81 mg daily. Per hematology note:
- “Weekly hematology follow-up for now”
- “Defer rituximab due to limited data w/ regard to safety in pregnancy. We could consider this if a future relapse occurs.”
Repeat ADAMTS13 activity levels:

She delivered a healthy baby boy at 36 weeks gestation without evidence of recurrence/relapse of TTP.