Case of polycythemia
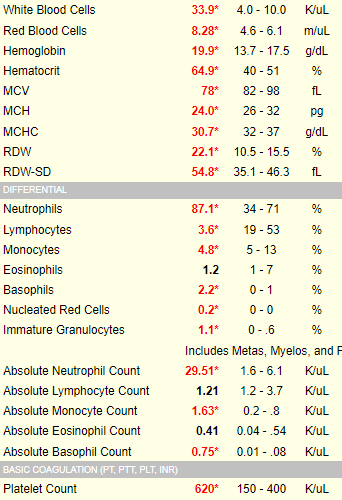
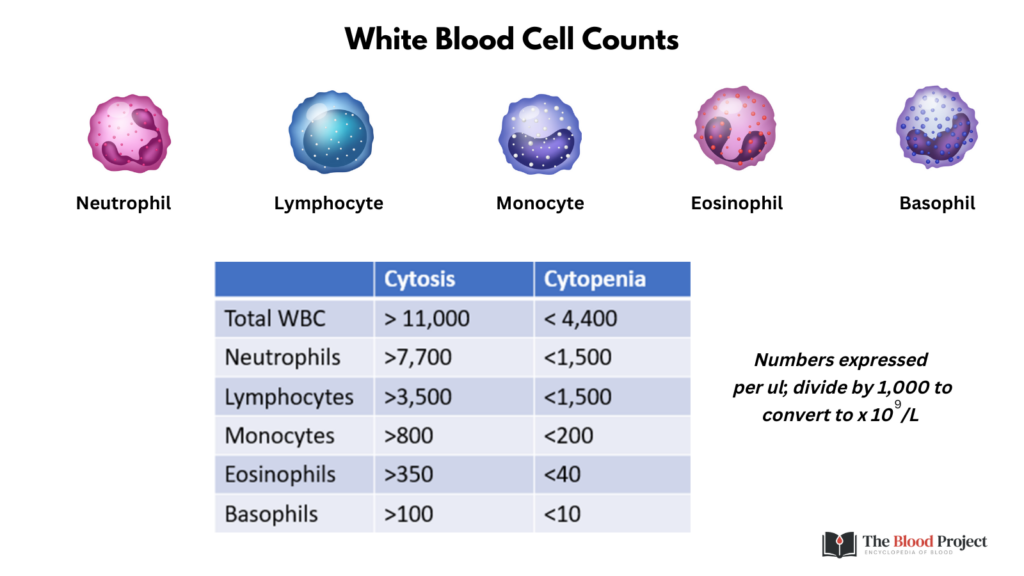
How do we know what qualifies for lower- or higher-than-normal white cell counts? Consult a cheat sheet like this one!
Before we get to the Twitter questions, let’s consider the definition and classification/differential diagnosis of polycythemia:
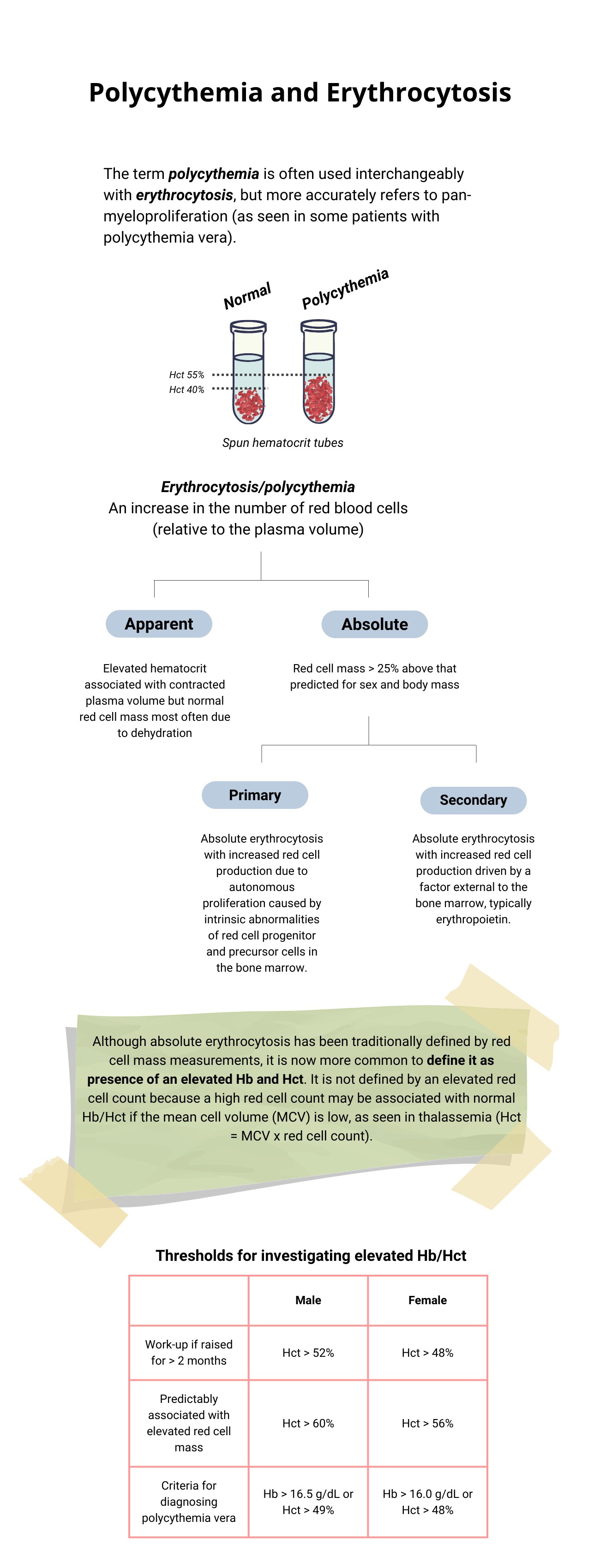
Definitions
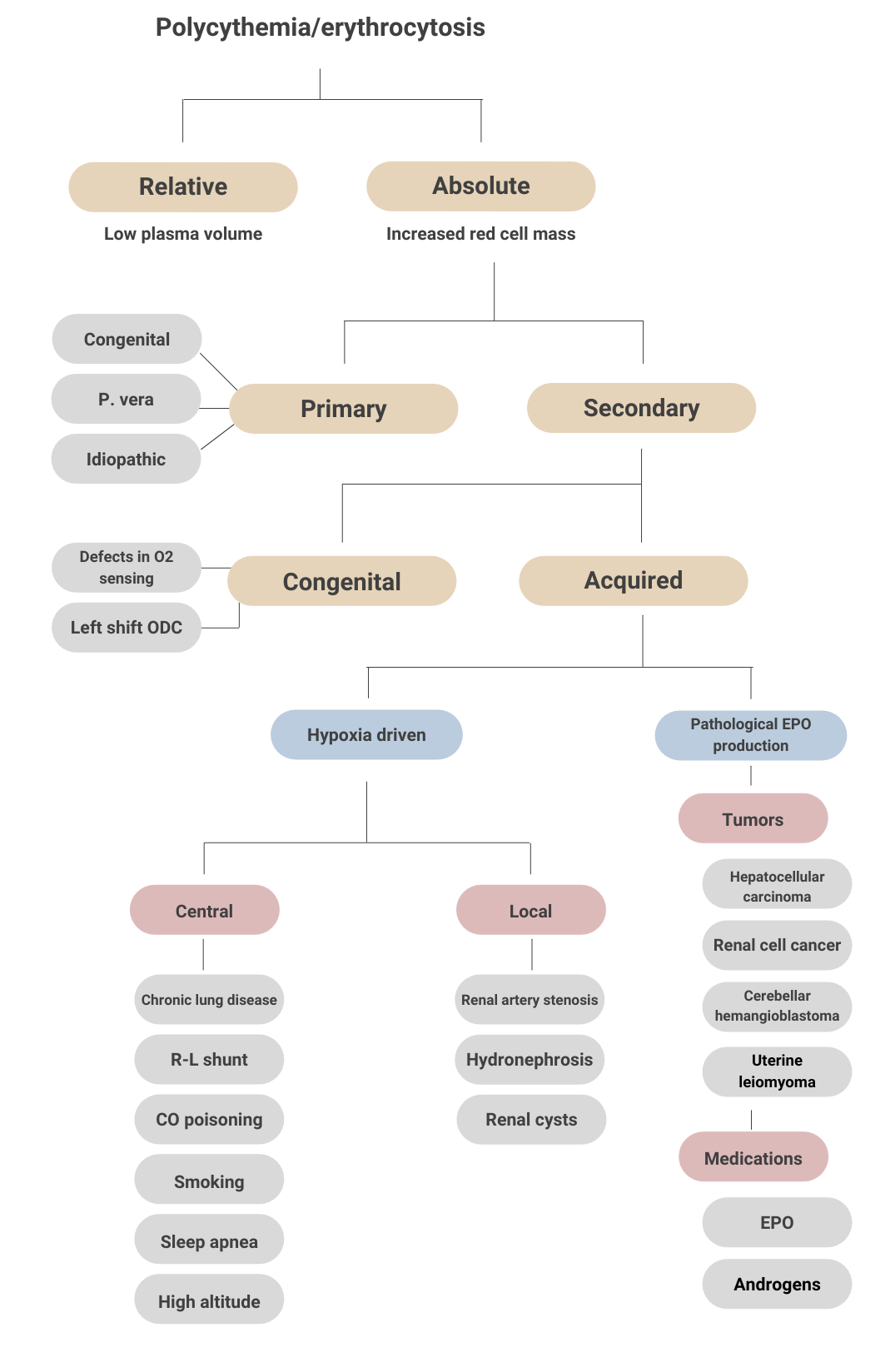
Classification
The color of the skin in cases of polycythemia vera is due largely to:
- The large increase in the circulating red blood cells and hemoglobin.
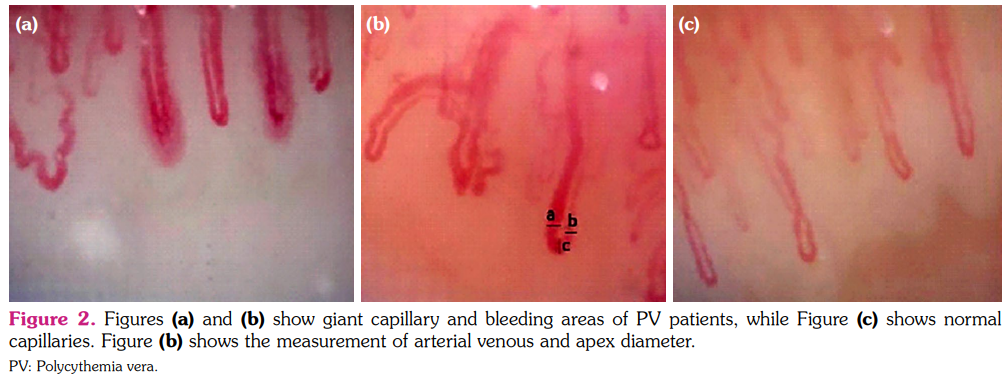
- The number of capillaries for each unit area of skin.
- The degree of vasodilation of skin microvessels.
What is the hemodynamic advantage of vasodilation in a patient with polycythemia vera?
Click for Answer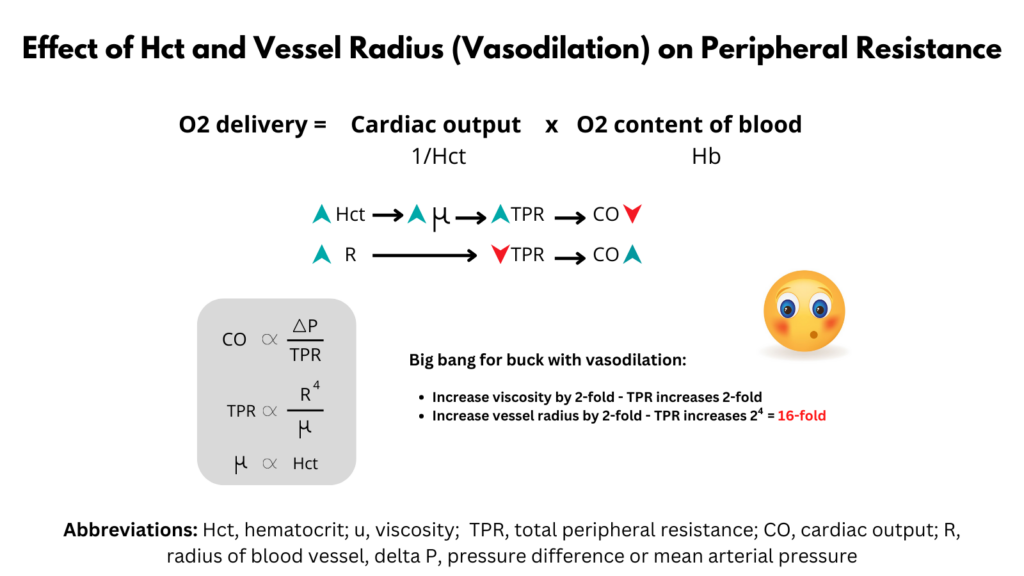
Is this patient or one with anemia more likely to develop cyanosis at a given SaO2?
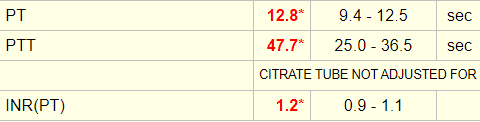
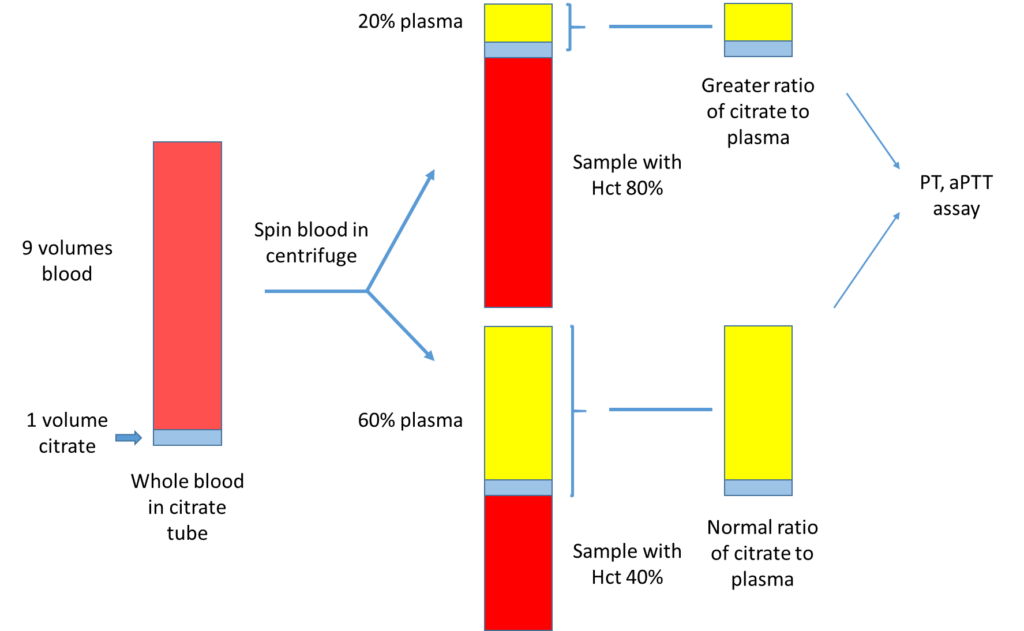
Click for AnswerThe patient’s initial coagulation screen showed the following:
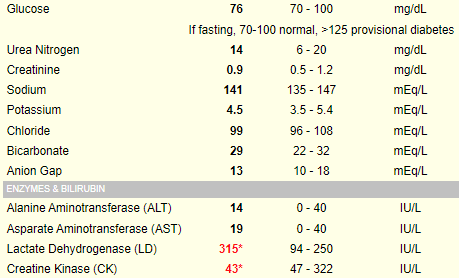
Serum lactate dehydrogenase (LDH) is a surrogate quantitative measure of cell turnover and tumor burden. The following is an abstract that reported the LDH level in 216 patients with polycythemia vera:

What single lab test would you like to order to definitively rule in/out polycythemia vera?
Click for AnswerHere are the results of the Jak2 mutations status:
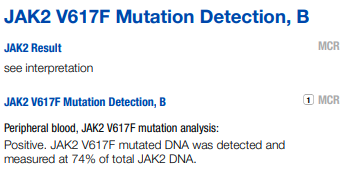
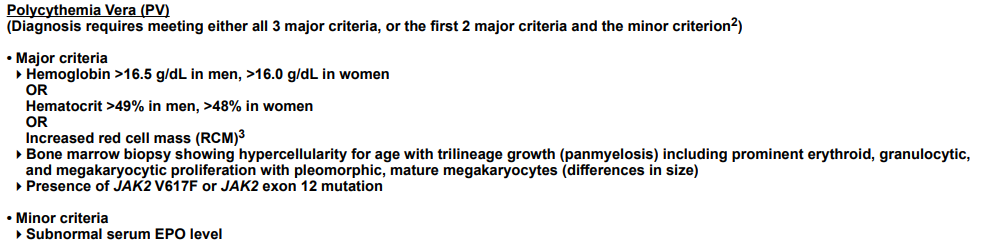
Our patient has 2 major criteria (Hb > 16.5) and presence of Jak2 V617F. For formal diagnosis, he would require a bone marrow biopsy. However, the pretest probability for polycythemia vera is virtually 100% and the patient should be treated accordingly.