Treatment

Let’s return to the concept of critical oxygen delivery. Recall the plot of oxygen delivery against oxygen consumption. Our patient, even with the most efficient of cardiovascular adaptations, will be squarely on the supply-dependent part of the curve. This means that any further reduction in oxygen delivery will lead to anaerobic metabolism and increased lactic acid production.
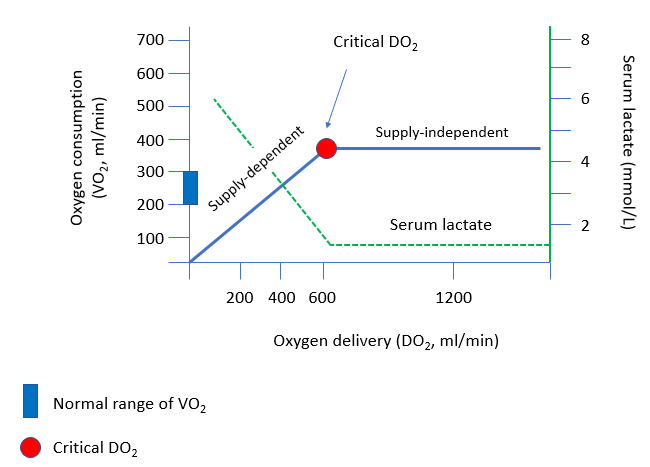
The surest way to offset this risk is to transfuse the patient. However, some patients, such as Jehovah Witnesses, do not accept blood transfusions. How would you manage a case such as this without transfusion support (see next slide for answer)?
Additional history from the patient’s family confirmed that the patient had experienced years long history of chronic abnormal uterine bleeding. A CTAP showed massively enlarged uterus measuring 17.8 x 12.0 x 15.4 cm, which was hyperenhancing and concerning for malignancy:
She ultimately had a EXPLORATORY LAPAROTOMY, TOTAL ABOMINAL HYSTERECTOMY, BILATERAL SALPINGO-OOPHORECTOMY, LYMPH NODE BIOPSY, which showed the following:
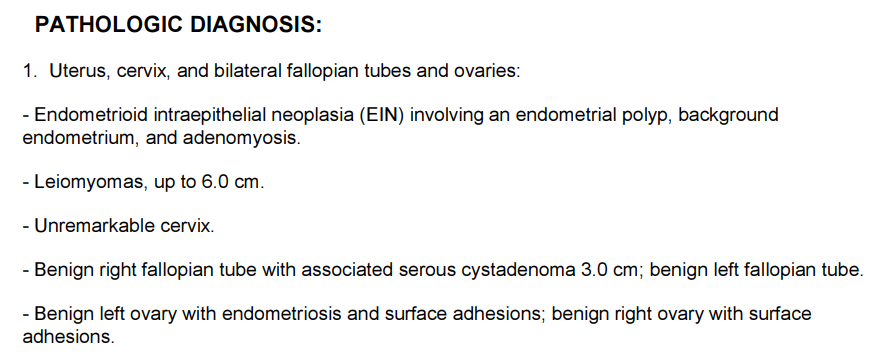
Thus, the diagnosis was fibroids.