Labs
Let’s begin with the patient’s complete blood count (CBC):
| WBC | Hb | MCV | PLT |
|---|---|---|---|
| 22.8 | 10.6 | 98 | 40 |
What’s what: WBC, white blood cell count; Hb, hemoglobin; MCV, mean cell volume; MCHC, mean cellular hemoglobin concentration; RDW-SD, red cell distribution width-standard deviation; platelets, PLT; Normal values: WBC 5-10 x 109/L, RBC 4-6 x 1012/L, Hb 12-16 g/dL, Hct 35-47%, MCV 80-100 fL, MCHC 32-36 g/dL, RDW-SD < 45%, platelets (PLT) 150-450 x 109/L
The following is the patient’s white cell differential:
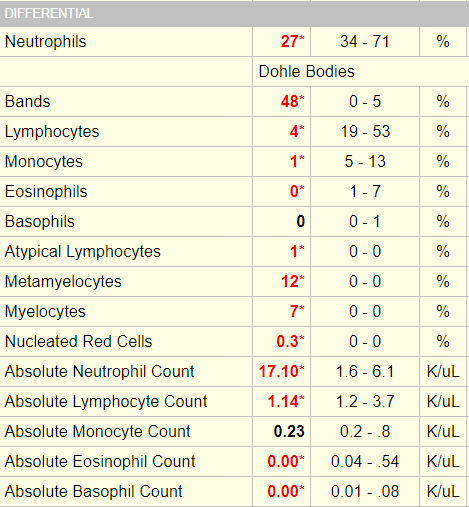
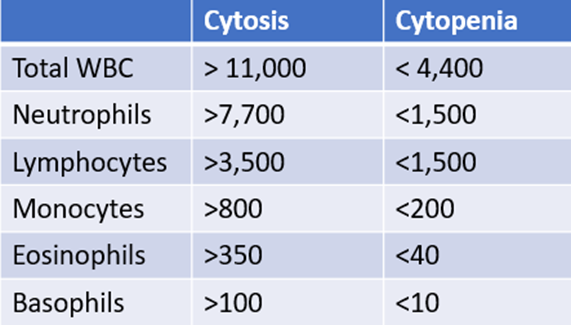
For mature white cells, it is advisable to focus on absolute counts rather than percentages because higher-than-normal or lower-than- normal counts are defined by thresholds in absolute numbers. This applies to those cell types that are enumerated by automated counters, namely neutrophils (which include segmented and band forms), lymphocytes, monocytes, eosinophils and basophils. To define which of the above counts are altered in our patient, we can refer to our “cheat sheet”:
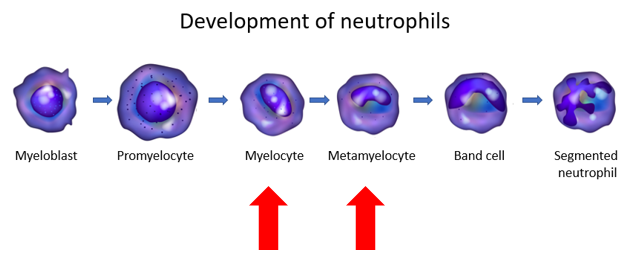
For less mature forms, namely myelocytes, metamyelocytes and promyelocytes in the granulocyte lineage, it is common practice to interpret the percentages relative to the total white cell count, because these are assessed by manual counting and because the presence of even a small number of these cells is abnormal.
What is a band neutrophil?
According to the College of American Pathologists:
- A band neutrophil is round to oval and 10 microns – 18 microns in diameter.
- The nuclear:cytoplasmic ratio is 1:1:5 to 1:2 and the nuclear chromatin is condensed.
- The nucleus is indented to more than half the distance to the farthest nuclear margin, but in no area is the chromatin condensed to a single filament.
- The nucleus can assume many shapes, including:
- Band-like
- Sausage-like
- S-shaped
- C-shaped
- U-shaped
- The cytoplasm contains primarily specific (pink) granules.
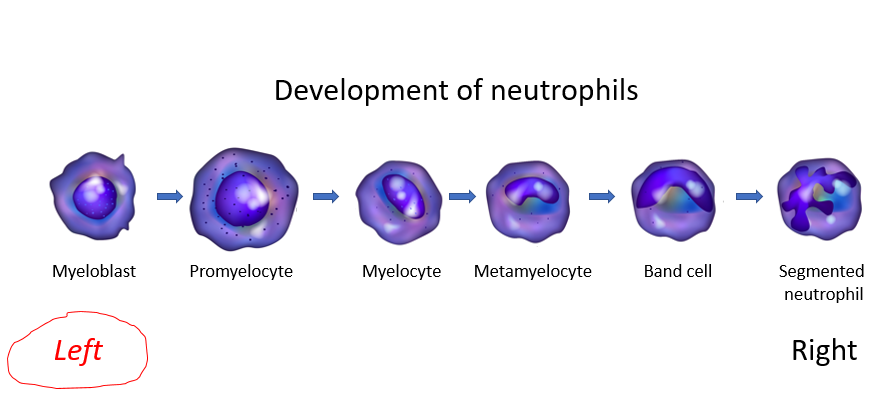
In addition to bands, the differential also showed increased numbers of metamyelocytes and myelocytes. These are less mature forms of granulocytes, situated further to the left on the differentiation schematic:
The patient’s differential showed neutrophilia, lymphopenia, and eosinopenia. This combination of changes is called a stress leukogram. It occurs in patients with stress of any kind, including in the setting of severe infection.
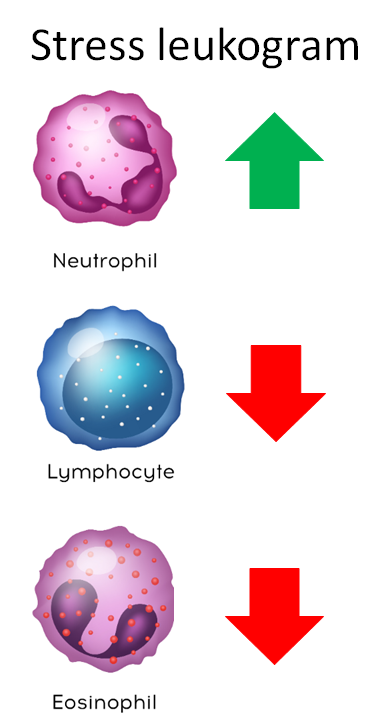
One way to remember this pattern is to consider that steroids (endogenous levels of which are increased in stress states) are used to treat lymphoma (by killing lymphocytes) and to treat hypereosinophilia (by killing eosinophils).
Monocyte counts tend to track with neutrophil counts in the stress response, but this is not always the case.
Let’s summarize the labs:
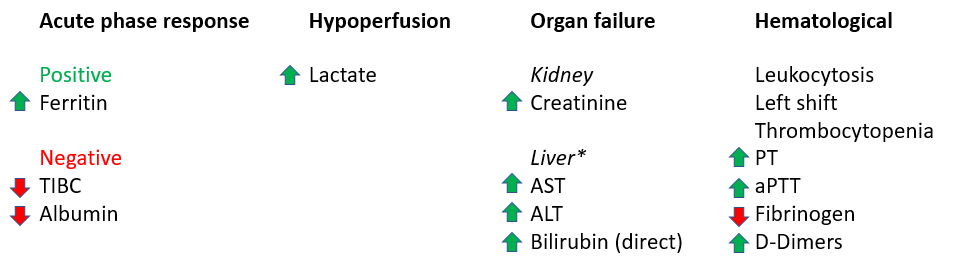
*To keep things simple, the patient’s liver function results are not shown, but they demonstrated evidence of shock liver with AST and ALT in the thousands IU, and a direct bilirubin that was was moderately elevated.
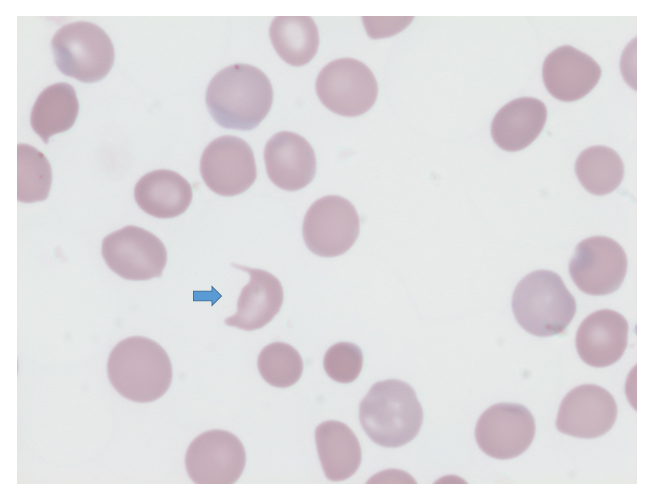
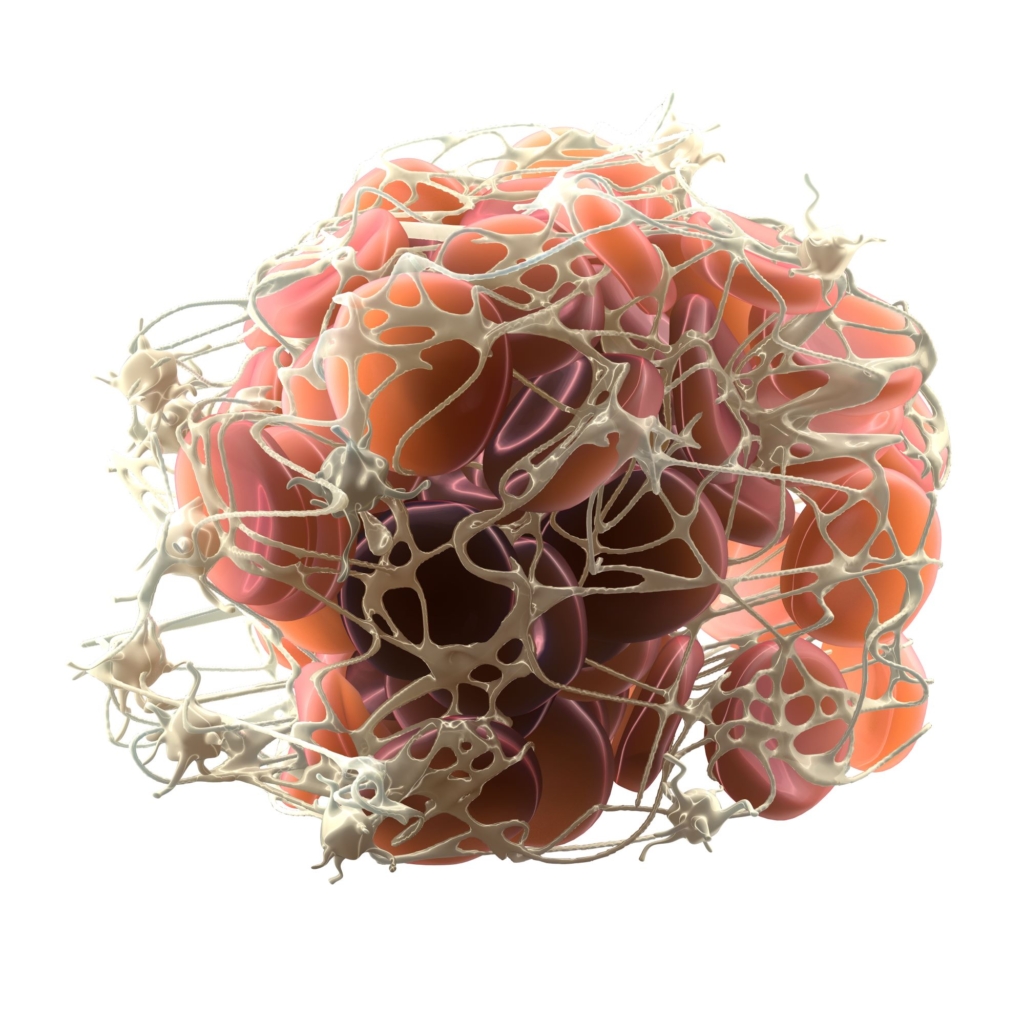
The patient’s peripheral smear shows presence of schistocytes, not unlike the following smear from a different patient.
The following are recommendations from two independent practice guidelines regarding the use of clinical scoring system:
Recommendation from the Harmonization guideline:

Recommendation from the Japanese Society of Thrombosis and Hemostasis :
Bottom line: Use an established scoring system to make the diagnosis.
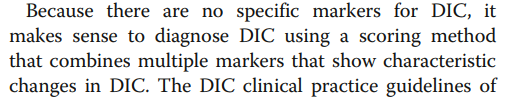
The following table shows a comparison of the commonly used diagnostic scoring systems for disseminated intravascular coagulation (DIC):
Note that for 2 of the 3 scoring systems (ISTH and JAAM), a diagnosis of DIC requires that patients have an underlying precipitating illness.
There are several common features and differences between these scoring systems:
Common features:
- All but one (JAAM) use the same 4 parameters:
- Platelet count
- Fibrin degradation products
- Fibrinogen
- Prothrombin time (PT)
Differences:
- Underlying disease is essential for ISTH and JAAM, but not for JMHW.
- Fibrinogen is graded for JMHW, but not ISTH. It is not included in the JAAM score.
- JAAM score takes into account the possibility that the platelet count is low in leukemia and other bone marrow disorders.
ISTH, International Society of Thrombosis and Haemostasis; JMWH, Japanese Ministry of Health and Welfare; JAAM, e Japanese Association for Acute Medicine; JSTH, Japanese Society of Thrombosis and Hemostasis; SISET, Italian Society for Thrombosis and Hemostasis
Fibrin-fibrinogen degradation products (FDPs), D-dimer
High sensitivity, low specificity (may be increased in cases of deep vein thrombosis, pulmonary thromboembolism, massive hydrothorax/ascites, and large subcutaneous hematomas).
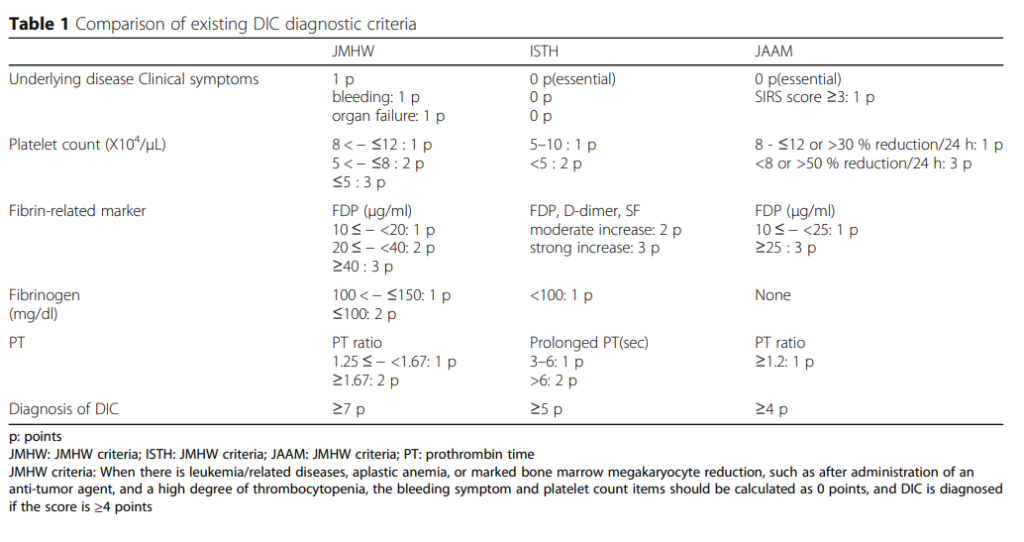
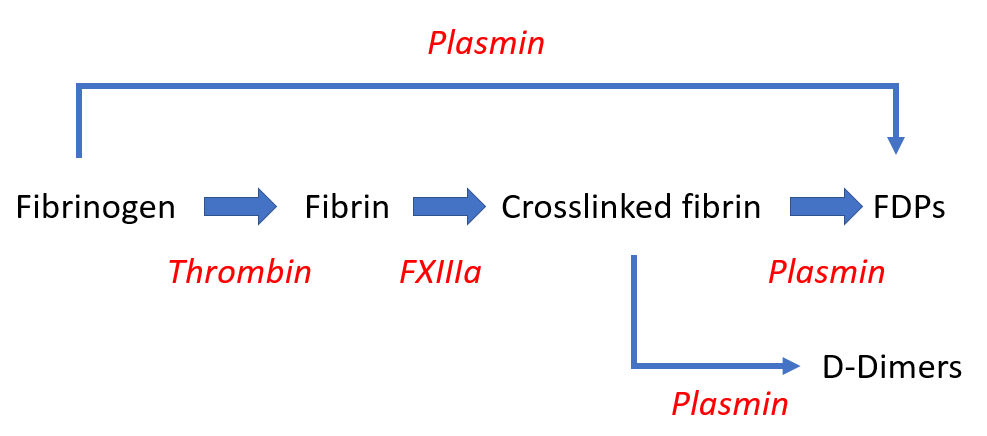
D-dimer:
- A degradation product of cross-linked fibrin.
- The smallest circulating FDP that is specific for fibrinolysis.
- Contains two cross-linked D fragments of the fibrin protein, hence its name.
- Quantified by immunoassay.
- Elevated in patients with disseminated intravascular coagulation (DIC), but high levels can also be found in patients with venous thromboembolism, recent surgery, or inflammatory conditions.
FDPs:
- FDP assays measure the breakdown split products of either fibrinogen or fibrin.
- Increased values indicate enhanced fibrinogenolysis or fibrinolysis.
- Quantified by immunoassay.
- Lacks specificity because in addition to DIC, high levels can be found with trauma, recent surgery, inflammation, venous thromboembolism, and many other conditions.
- Because FDPs are metabolized in the liver and cleared by the kidneys, levels are influenced by liver and kidney function.
Fibrinogen:
- Levels may decrease owing to consumption (increased conversion of fibrinogen to fibrin).
- Levels may be further decreased when there is predominant hyperfibrinolysis (which can result in direct cleavage of fibrinogen).
- Fibrinogen is an acute phase reactant, thus plasma levels may remain in normal range despite ongoing consumption.
- Low fibrinogen level has high specificity, but low sensitivity for disseminated intravascular coagulation (DIC).
- Overall sensitivity of low fibrinogen level reported to be only 28%, with hypofibrinogenemia occurring only in very severe cases of DIC.
- Not a diagnostic criteria in the JAAM score.
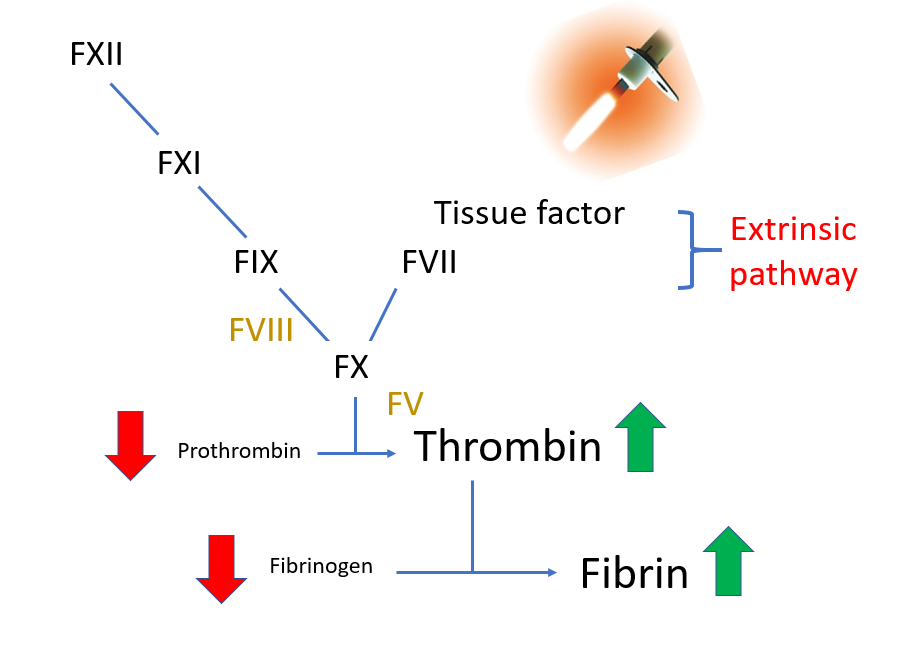
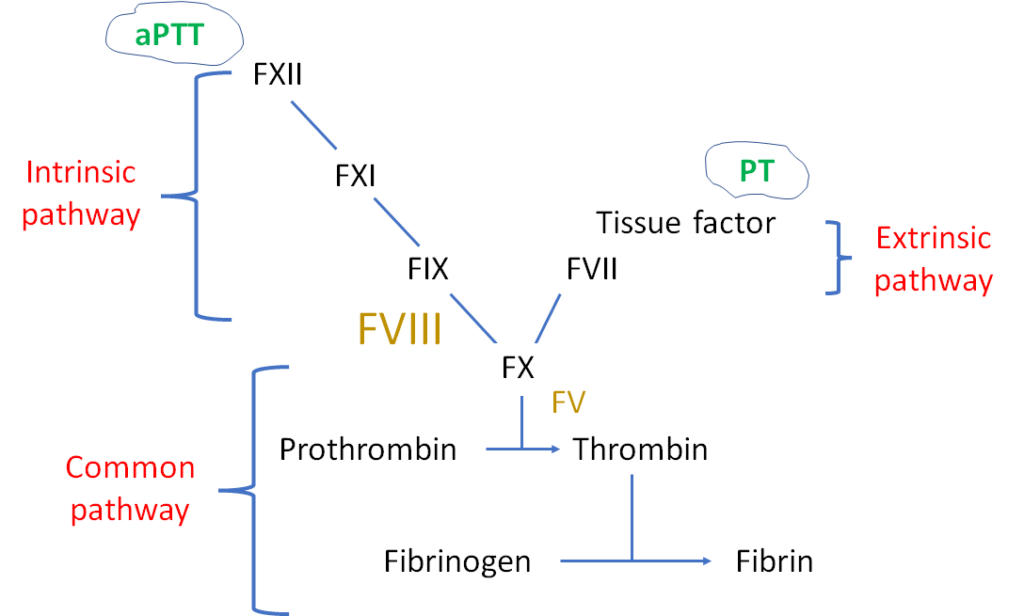
Prothrombin time (PT):
- Increased in about one-half patients with disseminated intravascular coagulation (DIC) at some point during the course of the disease.
- More sensitive than aPTT, which may be normal due to increased levels of factor VIII (FVIII), an acute phase reactant.
- Not specific for DIC; elevated PT also occurs in patients with congenital factor VII deficiency, liver disease and vitamin K deficiency.
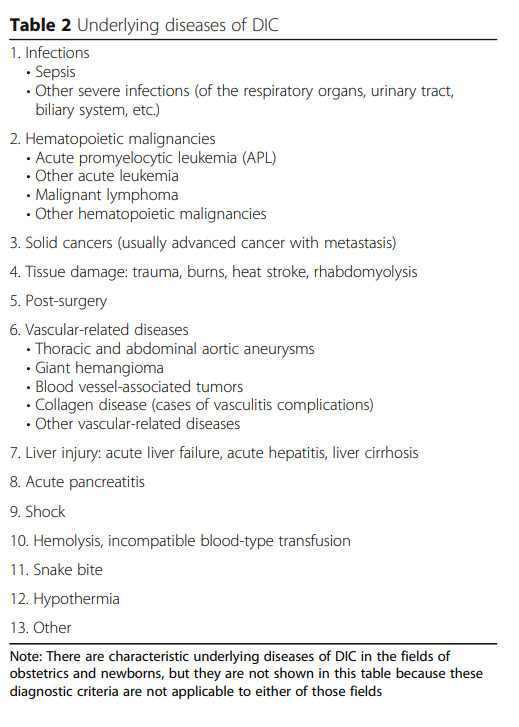
Recall that most guidelines require an underlying cause of disseminated intravascular coagulation (DIC). Here are some potential etiologies to look for:

To reiterate, DIC is diagnosed when the ISTH DIC score is 5 or higher:
Learn more about the ISTH DIC score:
- Original publication on the ISTH score can be found here.
- Prospective validation study can be found here – sensitivity of the DIC score 95%, specificity 98%.
- See ISTH calculator.