Labs
The following is the complete blood count (CBC) when the patient was first seen in the emergency room:
| WBC (109/L) | Hb (g/dL) | Hct (%) | MCV (fL) | PLT (109/L) |
|---|---|---|---|---|
| 33.9 | 20.8 | 69.3 | 81 | 632 |
What’s what: WBC, white blood cell count; Hb, hemoglobin; MCV, mean cell volume; MCHC, mean cellular hemoglobin concentration; RDW-SD, red cell distribution width-standard deviation; platelets, PLT; Normal values: WBC 5-10 x 109/L, RBC 4-6 x 1012/L, Hb 12-16 g/dL, Hct 35-47%, MCV 80-100 fL, MCHC 32-36 g/dL, RDW-SD < 45 fL, platelets (PLT) 150-450 x 109/L
If the patient’s mean cell volume was 95 fL six months ago, what would you be suspicious of today?
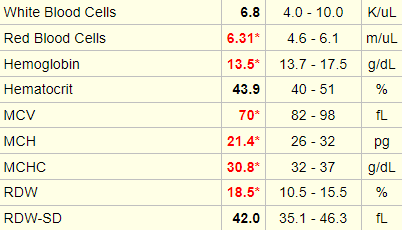
Click for AnswerThe following is a complete blood count from an individual with beta thalassemia. Note the increased red cell count, with a normal hematocrit (Hct). Hct = mean cell volume x red cell count, so if the red cells are small, as in this case, the bone marrow compensates by producing more of them to maintain a normal Hct. This condition used to be called microcytic erythrocytosis!
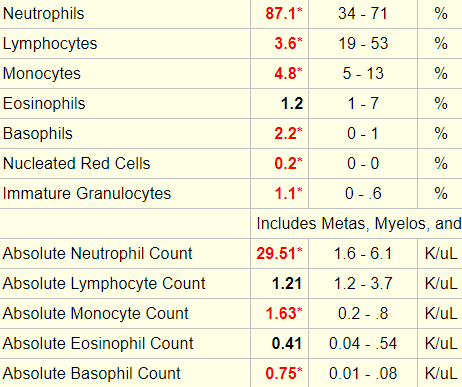
Let’s look at the white cell differential:

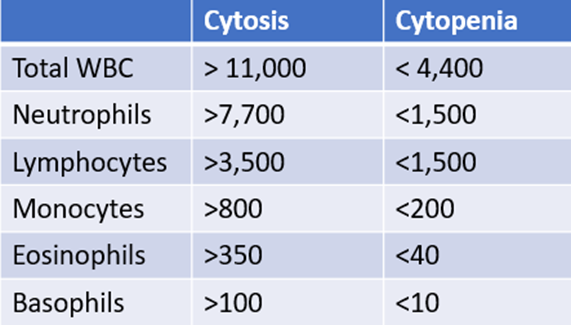
The following is “cheat sheet” of ranges that define lower- or higher-than-normal counts:
Why are the white cell counts and platelet count often elevated in polycythemia vera
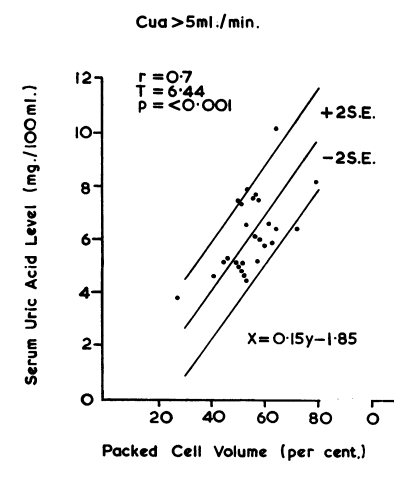
Click for AnswerHigh uric acid (complicated by gout and kidney stones) is associated with polycythemia vera due to the high turnover of red blood cells, which results in higher-than-normal uric acid production.
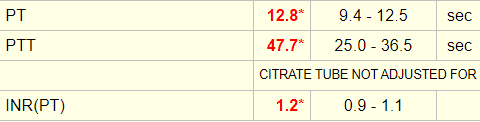
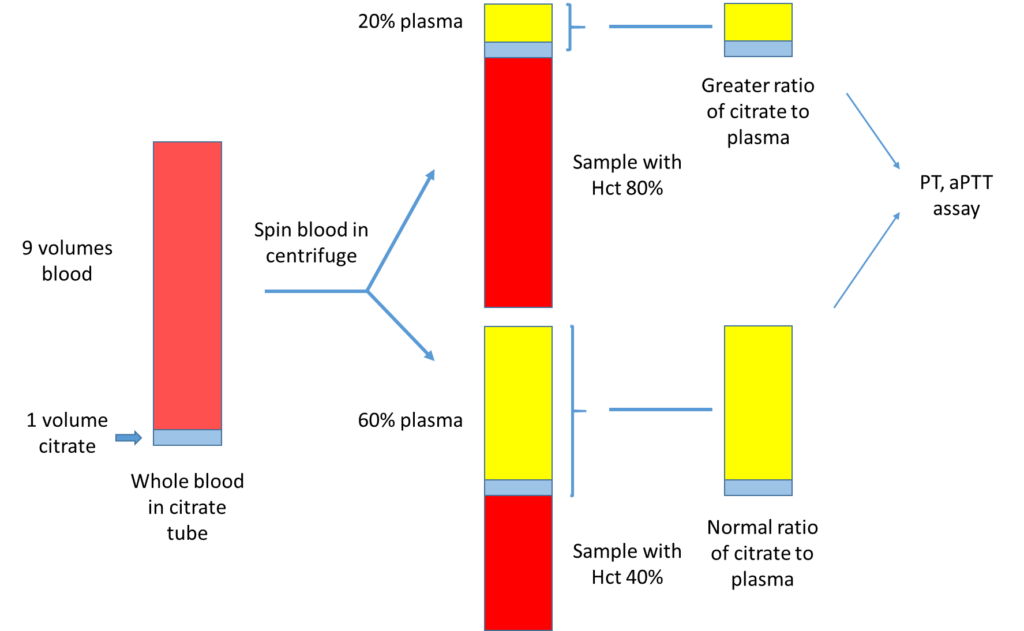
The patient’s initial coagulation screen showed the following:
Serum lactate dehydrogenase (LDH) is a surrogate quantitative measure of cell turnover and tumor burden. The following is an abstract that reported the LDH level in 216 patients with polycythemia vera:

What single lab test would you like to order to definitively rule in/out polycythemia vera?
Click for AnswerThe Jak2 mutation was ordered when the patient was first seen, but this test takes several days to come back, so treatment decisions had to be made without knowledge of the result.
When the test result did return, it showed the following:
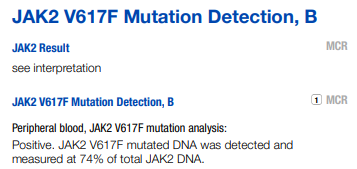
The erythropoietin level was undetectable!
