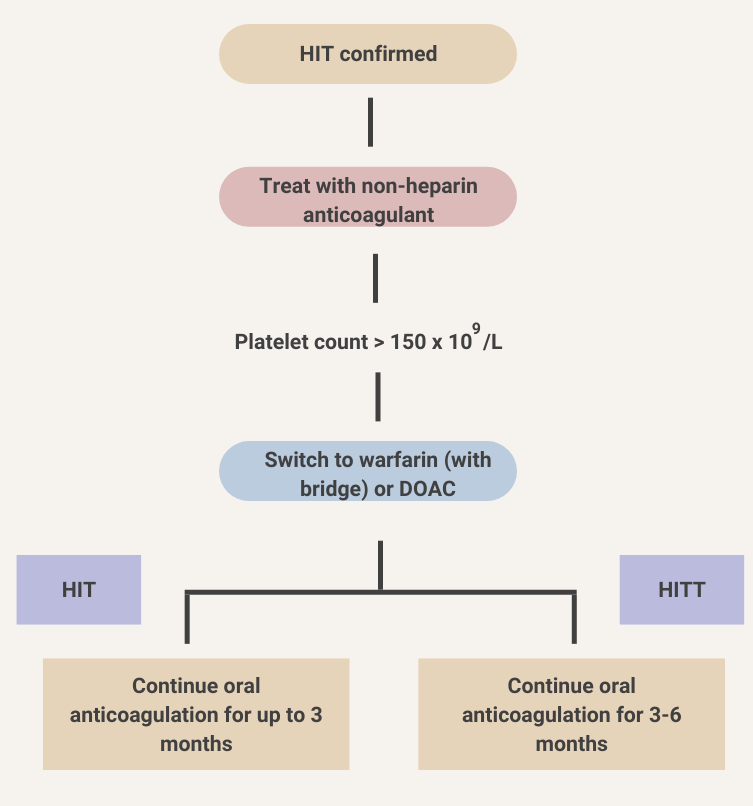
Treatment

Returning to a schematic we saw in the Labs section, the results of the 4T score determine the course of action not only with regard to further investigation (immunoassay) but also with regard to management (continue or stop heparin). If heparin is stopped, an alternative non-heparin anticoagulant must be started.
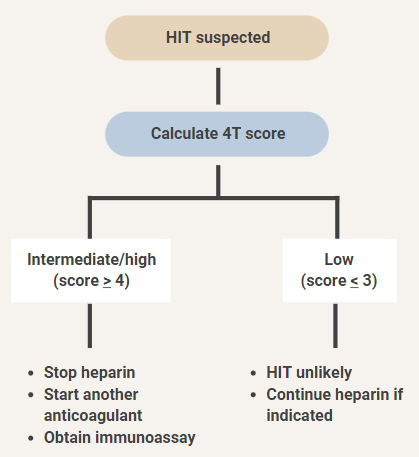
Our patient had a 4T score of 6. As we discussed in the section on labs, blood should be sent for an immunoassay. In addition, heparin should be discontinued, and a suitable anticoagulant started in its place.
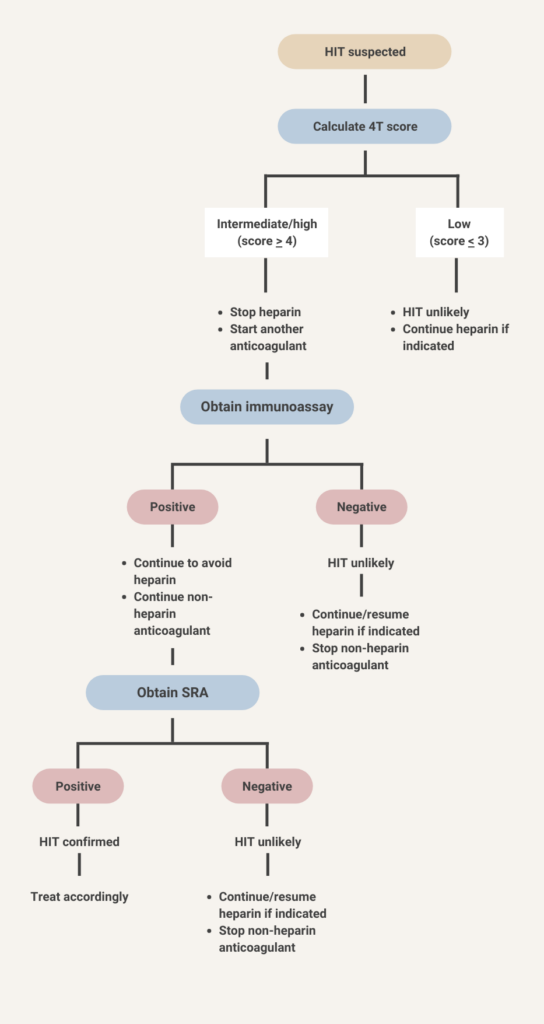
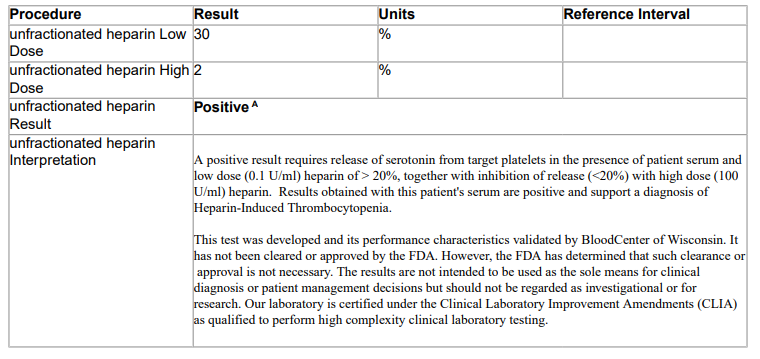
The serotonin release assay comes back positive. This patient’s actual result is shown below:

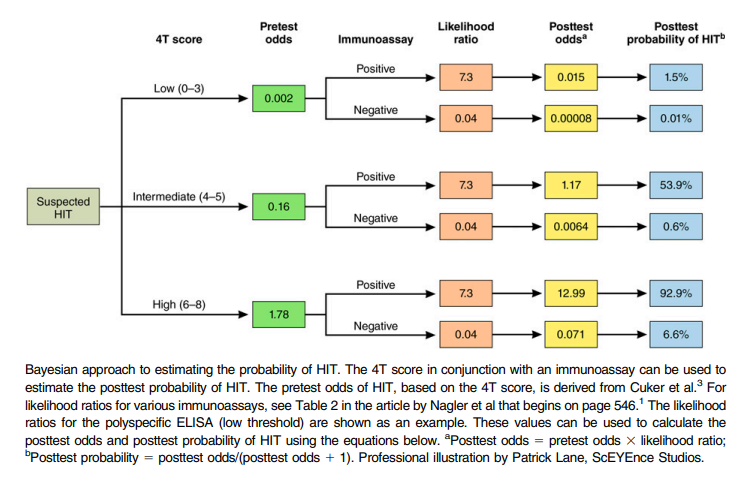
You may run into the terms pretest probability and post-test probability in the heparin-induced thrombocytopenia (HIT) literature.
- The pretest probability is the probability of having HIT based on the initial 4T score. For example, patients with a score of 6 or higher (such as our patient) have a high pretest probability (> 60%) of having HIT.
- The post-test probability is the probability of having HIT (as diagnosed by the gold standard serotonin release assay) based on the results of the immunoassay.