About the Condition
Description/definition:
Microcytic anemias are among the most common types of anemia encountered by physicians in general hospitals and outpatient clinics. Iron deficiency anemia and thalassemia minor are the most common causes of microcytic anemia.
It can sometimes be challenging to differentiate between iron deficiency anemia and thalassemia trait/minor, both causes of microcytic anemia. And, of course, both conditions may occur in the same patient.
It has been estimated that 30% of the global population suffers from iron deficiency anemia. 1.5% of the world’s population carries genes for beta thalassemia.
Traditionally, thalassemia was endemic in the “thalassemia belt” that extends from the Mediterranean basin via the Middle East, the Arabian peninsula, and the Indian subcontinent to Southeast Asia. However, global migration has now spread the disease through all continents.
Individuals with iron deficiency anemia are frequently symptomatic while those with thalassemia trait are usually asymptomatic and may be unaware of their carrier status.

Pathophysiology:
Iron deficiency anemia is caused by deficient delivery of iron to erythropoietic cells in the bone marrow, resulting in microcytosis and anemia.
Microcytic anemia in individuals with thalassemia results from impaired globin chain synthesis and decreased hemoglobin synthesis, resulting in microcytosis.
Diagnosis:
Red cell indices to predict iron deficiency vs. thalassemia minor:
- In the early 1970s, various hematologists pioneered the development of mathematical formulas that could successfully differentiate between thalassemia and iron deficiency anemia, using parameters obtained from automated blood counters.
- Many indices have been defined to quickly discriminate iron deficiency anemia from thalassemia. Currently, more than 45 such simple formulas are available!
- The purpose of using these indices is to:
- Detect subjects who have a high probability of requiring appropriate follow-up.
- Reduce unnecessary investigative costs.
- Avoid giving iron unnecessarily to an individual with thalassemia.
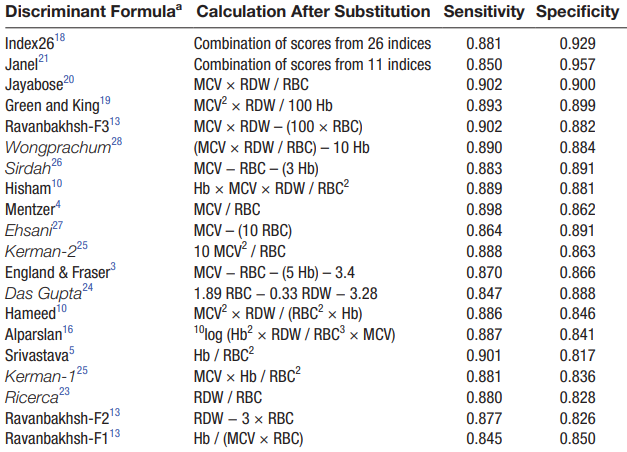
- None of the indices aimed to discriminate between these two conditions has 100% sensitivity and specificity.
The following are the 20 overall best-performing discriminant formulas:
Confirm diagnosis of iron deficiency or thalassemia minor:
- Serum ferritin – < 10 ng/ml is diagnostic of iron deficiency.
- Hb electrophoresis:
- Increased HbA2 in beta thalassemia trait
- Normal in alpha thalassemia trait
- Molecular testing – targeted polymerase chain reaction (PCR)-based mutation analysis to identify alpha thalassemia trait.
Treatment:
Iron deficiency anemia is treated with iron replacement (and transfusions if the degree of anemia is severe).
Thalassemia trait is a normal variant and does not require treatment.