Workings backward from an elevated MCV
The patient has an MCV of 121 fL.
The patient’s physical exam shows a swollen right leg from the ankle to the top of the thigh, similar to the image below (showing right calf).

This is what you have been waiting for… the patient’s complete blood count (CBC)!
| WBC (109/L) | Hb (g/dL) | MCV (fL) | RDW-SD (fL) | PLT (109/L) |
|---|---|---|---|---|
| 5.7 | 9.5 | 120 | 67 | 154 |
What’s what: WBC, white blood cell count; Hb, hemoglobin; MCV, mean cell volume; MCHC, mean cellular hemoglobin concentration; RDW-SD, red cell distribution width-standard deviation; platelets, PLT; Normal values: WBC 5-10 x 109/L, RBC 4-6 x 1012/L, Hb 12-16 g/dL, Hct 35-47%, MCV 80-100 fL, MCHC 32-36 g/dL, RDW-SD < 45 fL, platelets (PLT) 150-450 x 109/L
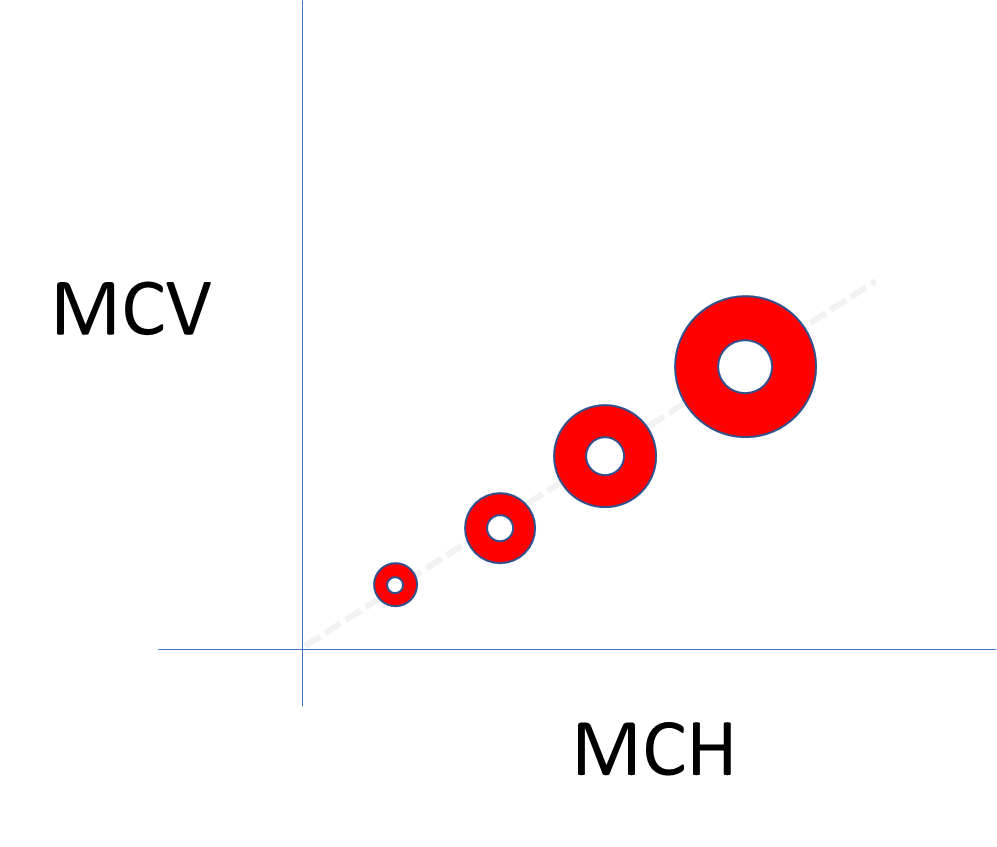
Note that the mean corpuscular hemoglobin (MCH) is not provided in the CBC above. Why? Because it really does not add anything.
Relationship between MCH and MCV (assuming a constant MCHC):
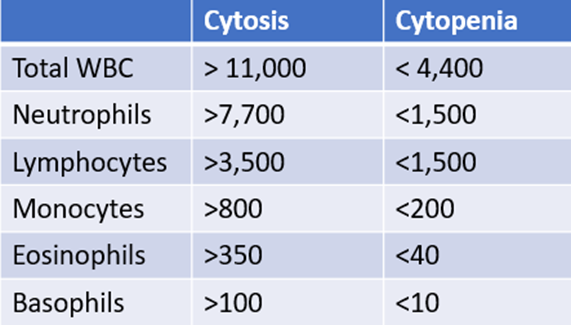
The following three slides show examples of a normal white cell count with an abnormal differential. To properly interpret these data, we need a ‘cheat sheet’ of threshold values, which is included with each example. The white cell differential is expressed in two ways: as a percentage of the total white cell count (e.g., neutrophils constitute 60% of 5 x 109/L white cells) or as an absolute number (e.g., the absolute number of neutrophils is 60% x 5 x 109/L white cells = 3.0 109/L). When considering the 5 normal white cell subsets, focus on the absolute counts. Why? Because an elevation (cytosis) or reduction (cytopenia) in counts is defined by deviation in absolute counts!

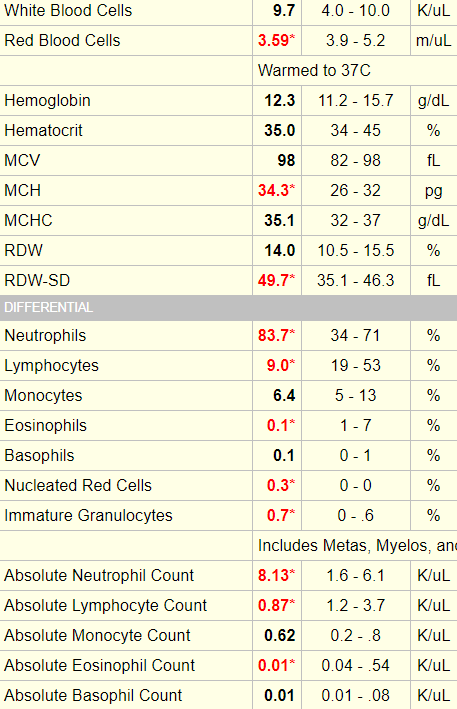
Example 1
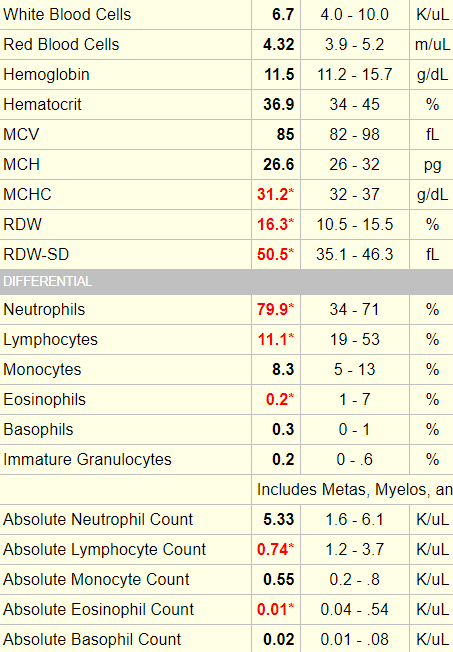
Example 2
Example 3
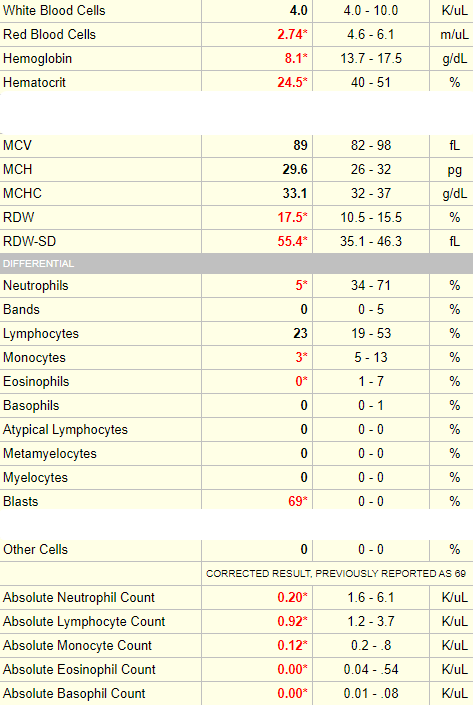
Note that in this case, blasts are reported only as a percentage of the total white cell count. While it is advisable to consider absolute counts for mature cells (neutrophils, lymphocytes, monocytes, eosinophils and basophils), it is common practice to refer to the percentage of immature white cells (including bands, metamyelocytes and myelocytes, promyelocytes and blasts) because if they are present, they are usually at low numbers (though in this case, the blast count is VERY high and could easily be converted into a meaningful absolute count).
Let’s return to our patient. Here is his white cell differential:
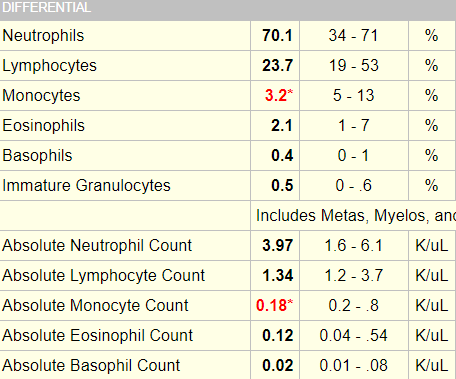
In this case, the patient’s differential is normal with the exception of a slight non-specific reduction in monocyte counts.
What is the next test you would like to order (not including the peripheral smear)?
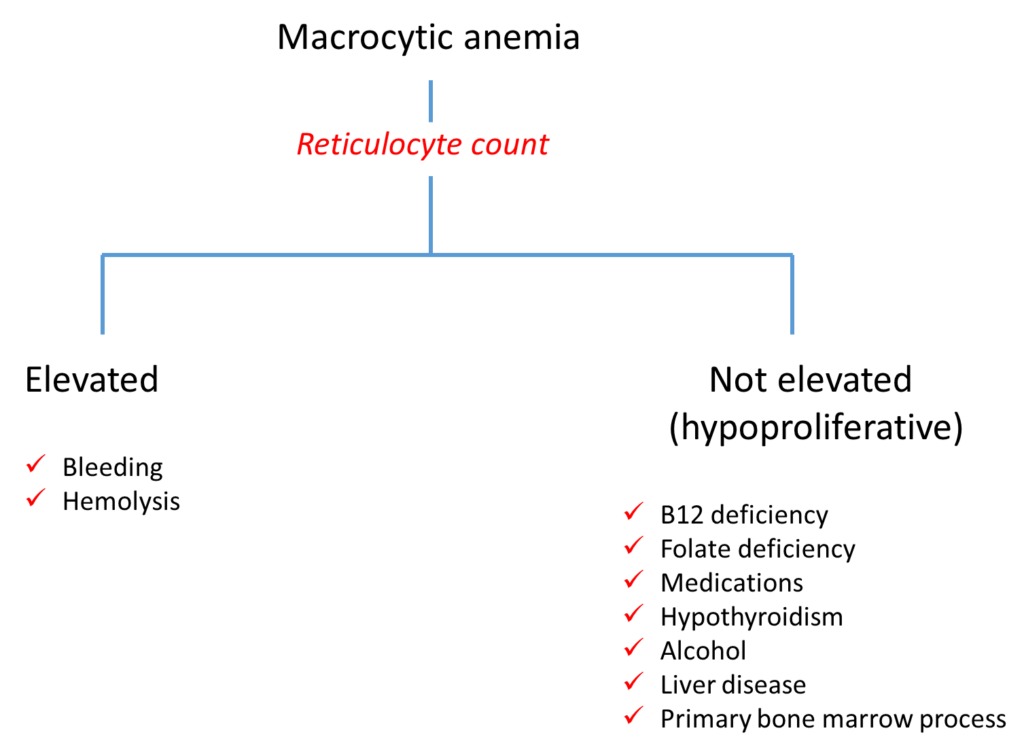
Click for AnswerThat’s right, the reticulocyte count is the first branch point in the diagnostic algorithm for macrocytic anemia!
Here is the patient’s reticulocyte count, expressed as a percentage of red cells and as an absolute count:

As we discussed earlier for the white cell count, the absolute number of reticulocytes provides more useful information than the percentage (which requires a fudge factor to account for the degree of anemia).
As a general rule of thumb, a reticulocyte count > 120 x 109/L is an appropriate bone marrow response to anemia.
In this case, the absolute reticulocyte is reported as 0.07 m/uL, which is 0.07 x 1012/L or 70 x 109/L. Thus, this patient has an inappropriate reticulocyte response. The anemia is defined as hypoproliferative.
There is no evidence of liver disease, and there is no history of hematoma, dark urine or jaundice. You find the additional lab results:
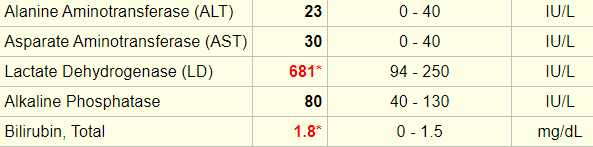
Let’s explore the diagnostic algorithm for hemolysis (we’ll get to the peripheral smear shortly!).
Here is one way to classify hemolytic anemia:
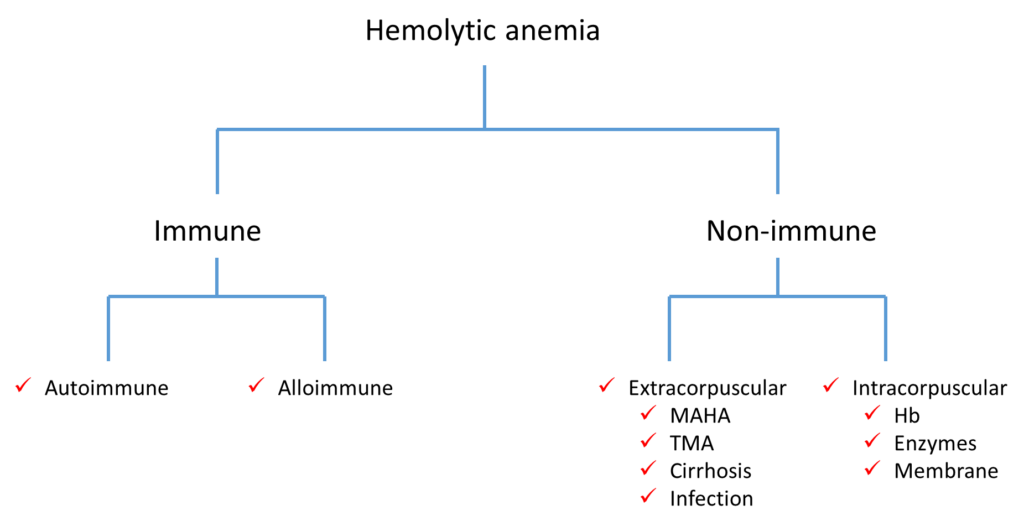
If you replace the term hemolytic anemia at the top of the algorithm with positive hemolytic markers, what other types of conditions would you add to this scheme?
Now we can take a look at the peripheral smear:
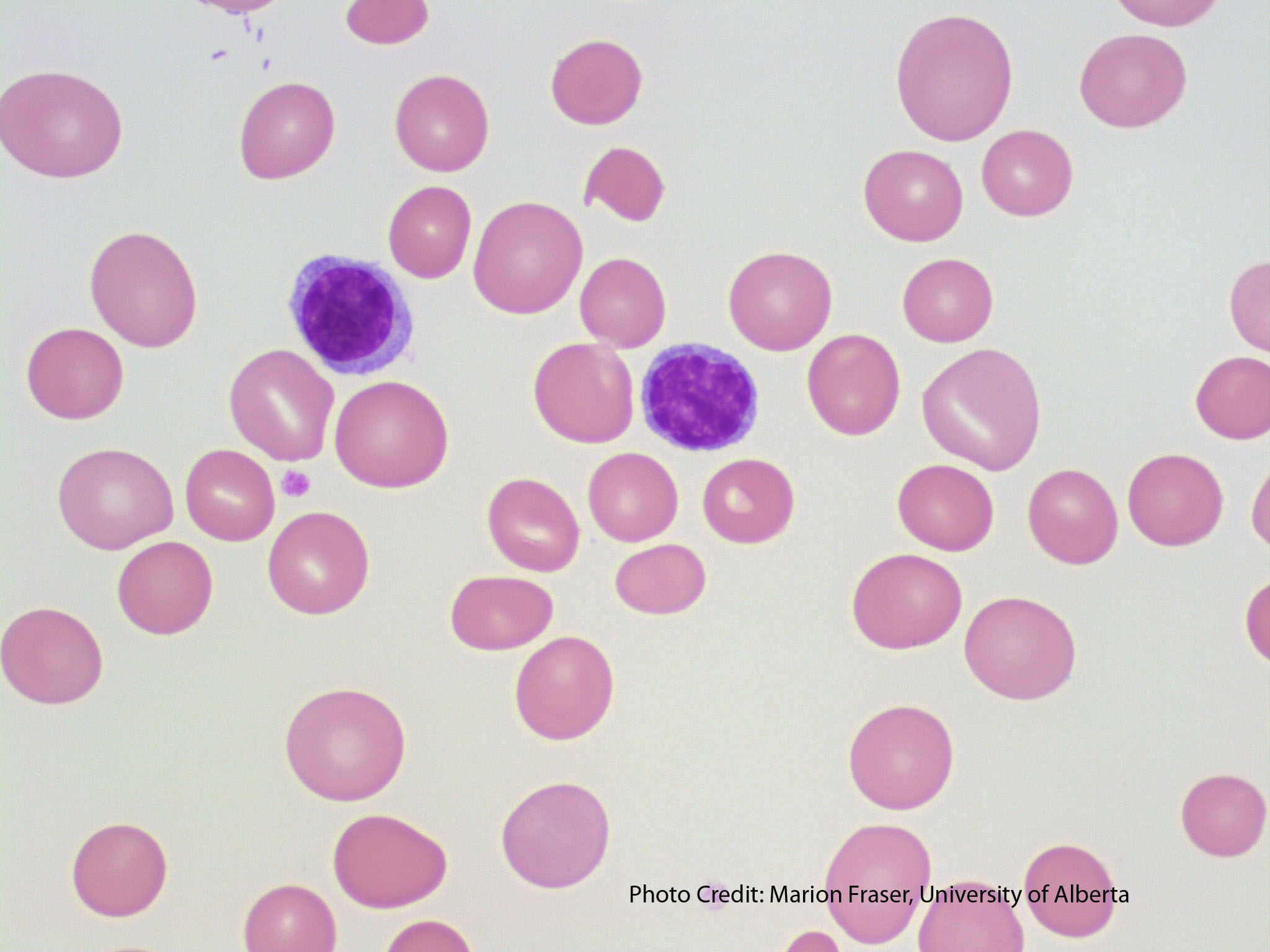
The peripheral smear of this patient was similar to the one shown above. There were lots of macro-ovalocytes and occasional fragmented red cells.
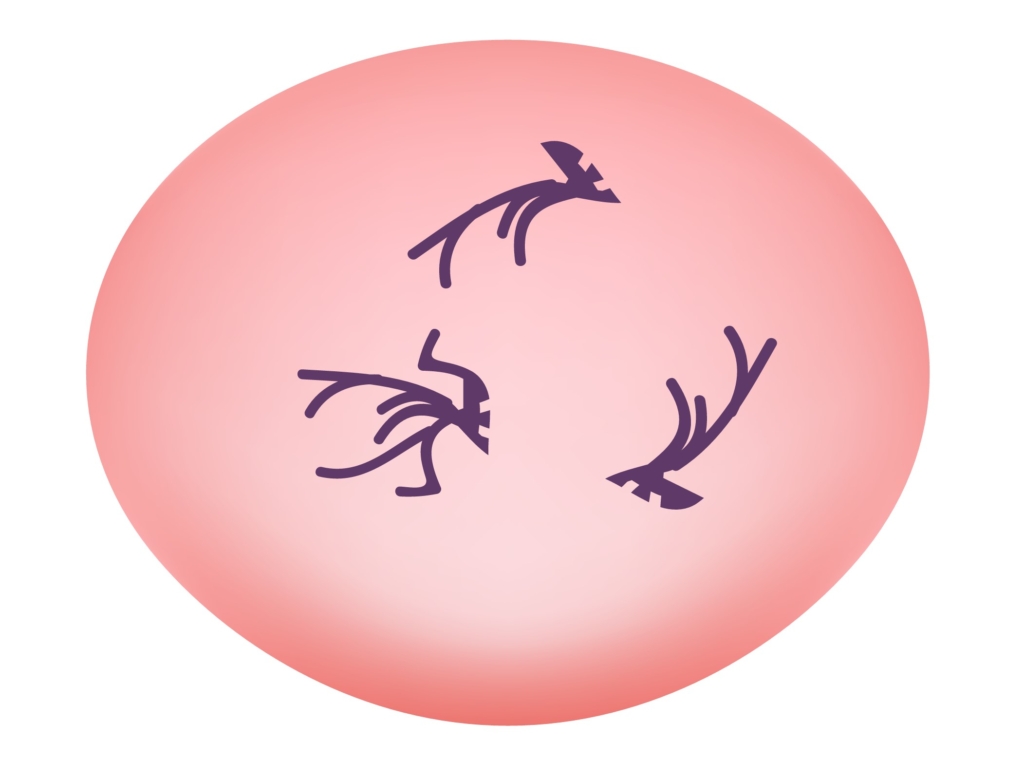
The peripheral smear also showed occasional hypersegmented neutrophils, similar to the image below:
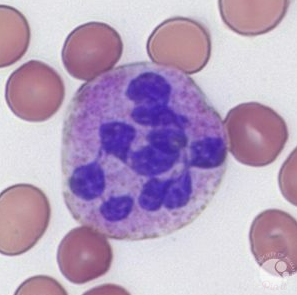
Hypersegmented neutrophils:
- Suggested by > 5% of neutrophils with ≥ 5 lobes or 1% with 6 lobes.
- Supports diagnosis of megaloblastic anemia (especially vitamin B12 and folate deficiency).
- Typically appear before macrocytosis and anemia.
Let’s return to the differential diagnosis of macrocytosis again:
- Increased reticulocytes
- Vitamin B12 deficiency
- Folate deficiency
- Medications
- Alcohol
- Liver disease
- Hypothyroidism
- Aplastic anemia
- Plasma cell dyscrasia
- Myelodysplastic syndrome
Here are the results of the patient’s serum vitamin B12 and folate:

Definition of vitamin B12 deficiency:
- British Committee for Standards in Haematology (BCSH) guideline suggests using cutoff of < 148 pmol/L (200 pg/mL) or cutoff derived from local reference range in patient with strong clinical suspicion of vitamin B12 deficiency.
- British Columbia (Canada) Medical Association suggests probability of vitamin B12 deficiency high with cutoff < 75 pmol/L (102 pg/mL), moderate with cutoff 75-150 pmol/L (102-203 pg/mL), low with cutoff > 150 pmol/L (203 pg/mL).
Serum vitamin B12 (cobalamin) level:
- Preferred initial test for detecting vitamin B12 deficiency.
- Assay measures both active form of cobalamin (holotranscobalamin) and inactive form (holohaptocorrin).
- Assay for measuring serum vitamin B12 is not standardized and there is no consensus cutoff to define deficiency.
We will come back to this figure in the next section (Pivoting from blood to stomach), but the important point to make here is that vitamin B12 is carried in the blood by two binding proteins (transcobalamin [TC] and haptocorrin [HC]), and only one of these (TC) carries bioavailable B12. The vitamin B12 test assays both TC- and HC-bound vitamin B12. Thus, high HC levels may mask B12 deficiency.

Are you familiar with functional assays for vitamin B12 deficiency? There are two of them.
The reason these two metabolites are increased in vitamin B12 deficiency is depicted in the following scheme which shows the two B12-dependent enzymatic reactions in the body:
- Methionine synthase reaction in the cytoplasm – conversion of homocysteine to methionine allows recycling of 5-methyl-tetrahydrolfolate (THF) to N5,10 methylene-THF which is necessary for generation of thymidylic acid, that is then used for DNA synthesis. Homocysteine levels build up when vitamin B12 levels are low.
- Methylmalonyl CoA mutase reaction in the mitochondria – conversion of methylmalonyl CoA (generated from propionic acid by bacteria-derived propionic acid) to succinyl CoA, a precursor for heme and fatty acid synthesis. Methylmalonic acid levels build up when vitamin B12 levels are low.
