When the A1c Doesn’t Fit the Patient
When the A1c Doesn’t Fit the Patient
An unexpected clue to compensated hemolysis
By William C. Aird, MD
Initial Laboratory Findings
Laboratory studies demonstrate evidence of hemolysis:
| Test | Result |
|---|---|
| Hemoglobin | 12.1 g/dL |
| Reticulocyte count | Elevated |
| Haptoglobin | <10 mg/dL |
| LDH | Elevated |
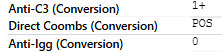
| Direct antiglobulin test | C3d positive, IgG negative |
| Cold agglutinin screen | Positive |
Example blood bank report:

Peripheral smear shows red cell clumping, and the MCHC is elevated.
Example peripheral smear:
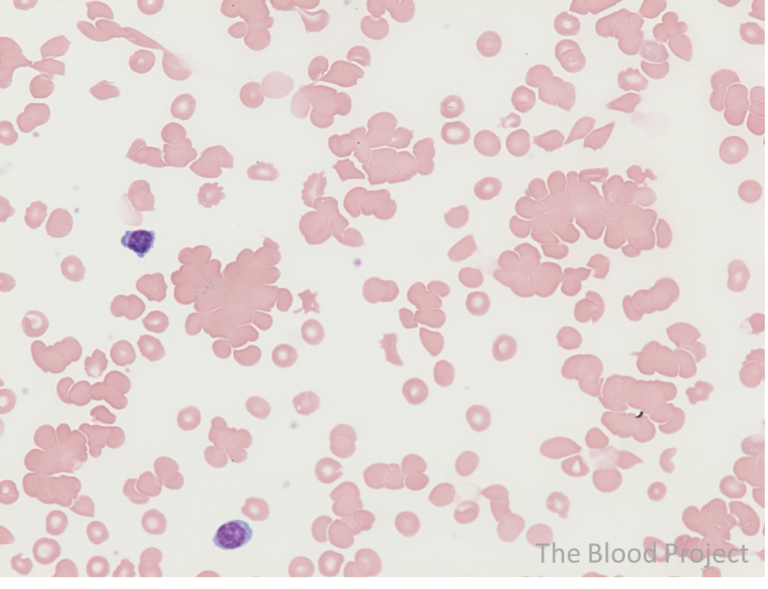
Cold agglutinins cause red cells to aggregate at lower temperatures. Automated analyzers may interpret clumped cells as single larger cells, which can artifactually elevate the MCHC. In this context, laboratory artifact itself becomes a diagnostic signal.