Labs
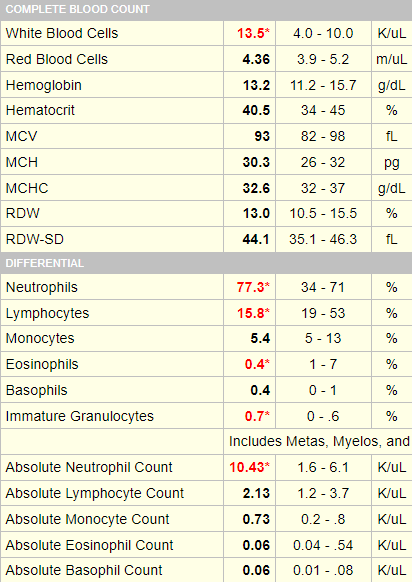
The following is the complete blood count (CBC) on the day you see the patient:
| WBC (109/L) | Hb (g/dL) | Hct (%) | MCV (fL) | PLT (109/L) |
|---|---|---|---|---|
| 13.5 | 13.2 | 40.5 | 93 | 303 |
What’s what: WBC, white blood cell count; Hb, hemoglobin; MCV, mean cell volume; MCHC, mean cellular hemoglobin concentration; RDW-SD, red cell distribution width-standard deviation; platelets, PLT; Normal values: WBC 5-10 x 109/L, RBC 4-6 x 1012/L, Hb 12-16 g/dL, Hct 35-47%, MCV 80-100 fL, MCHC 32-36 g/dL, RDW-SD < 45 fL, platelets (PLT) 150-450 x 109/L
Thus, the patient does indeed have leukocytosis.
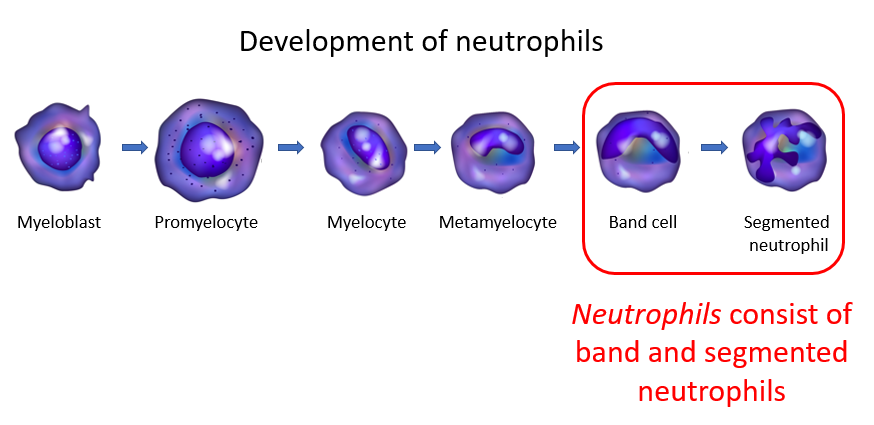
Automated differential

Manual differential

The white cell differential was carried out in this patient using an automated counter. The results are the following:

Here is an example from a different patient:
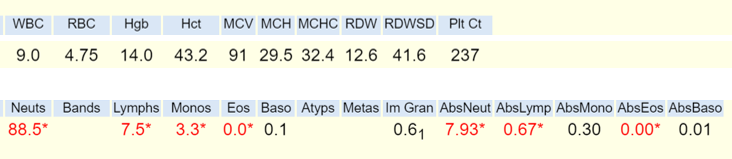
The learning point here is that a normal count can belie abnormalities in the differential, and we won’t know about these unless we look!