About the Condition
Description/definition:
Leukocytosis is defined as a total white cell count (WBC) > 11 x 109/L.
Neutrophilia is defined as an absolute neutrophil count > 7.7 x 109/L.
Association between smoking and leukocytosis/neutrophilia (“smoker’s leukocytosis”):
- Causal role supported by dose-response relationship, with a larger effect seen in heavier smokers, as well as the fact that smokers’ higher WBC counts reverse rapidly after smoking cessation (within 8 weeks).
- Some studies also show smaller increases in the counts of lymphocytes, monocytes, and eosinophils in smokers.

Pathophysiology:
Life cycle of neutrophils
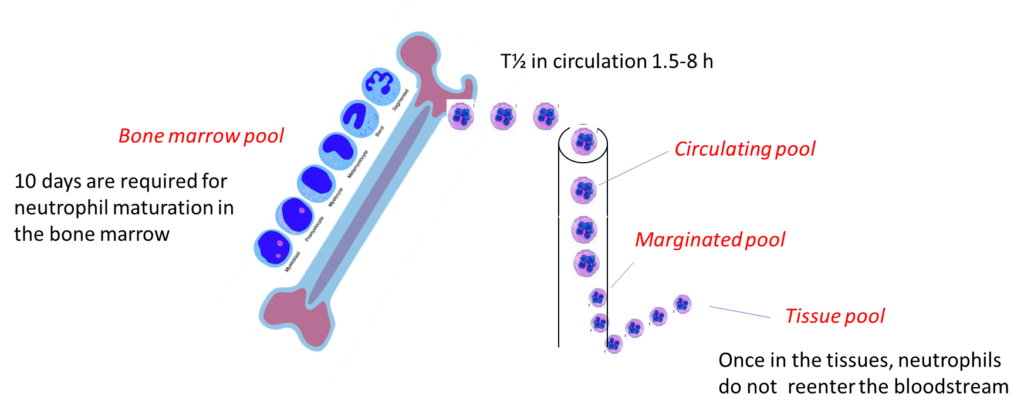
Neutrophils:
- Develop over a 14-day period in the bone marrow (bone marrow pool):
- Neutrophils (and their precursors) spend most of their life span in storage.
- Once neutrophils have matured within the bone marrow, 80% – 90% remain in storage.
- This large reserve allows for a rapid increase in the circulating neutrophil count within hours.
- Freely circulate in the peripheral blood for several hours (circulating pool, consisting of 2% to 3% of leukocytes).
- Bind to the endothelium (marginated pool).
- Egress (transmigrate) into tissues, where they survive 6–15 times longer than circulating neutrophils (tissue pool).
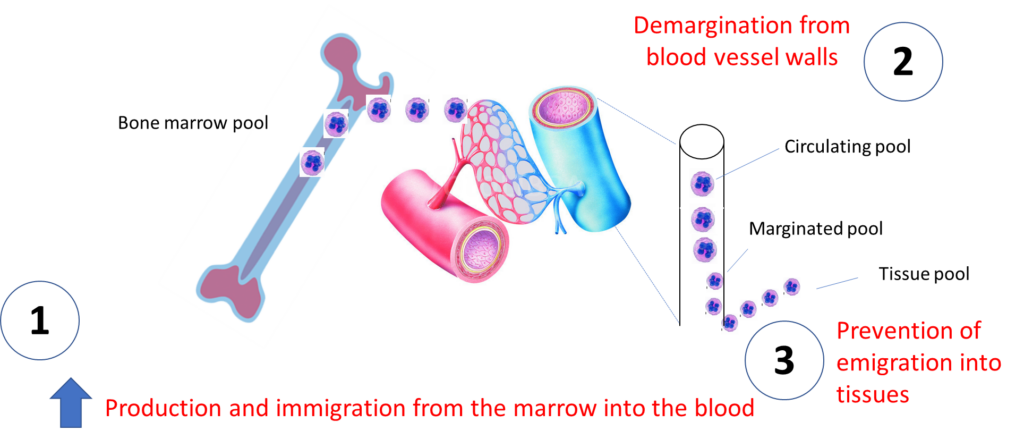
Mechanisms of neutrophilia:
- Increased production and immigration from marrow into blood
- Demargination from blood vessel walls
- Prevention of emigration into tissues
Mechanisms of smoking-associated neutrophilia are speculative:
- Induction of a chronic systemic inflammatory response resulting from:
- Irritation of the respiratory mucosa.
- Impaired function of alveolar macrophages, leading to decreased clearance of intracellular apoptotic material.
- Nicotine, a component of cigarette smoke, induces the release of catecholamines and promotes a rise in levels of cortisol, both of which are known to increase the leukocyte count.
- Smoking-related hemoconcentration, though the white cell count does not correlate with the Hb/Hct in smokers.
Clinical presentation:
Patients with neutrophilia cause may present:
- Incidentally or with symptoms:
- Typically associated with underlying cause of neutrophilia.
- Patients with hyperleukocytosis (white cell count > 100 x 109/L) and presence of immature white cells may present with symptoms of leukostasis.
- Acutely or with chronically elevated neutrophil counts.
- With isolated neutrophilia or with other abnormalities in the complete blood count.
Since the patient in this case study clearly had a reactive neutrophilia, we will limit our discussion to these causes:
| Cause | Comment |
|---|---|
| Infection | Typically bacterial infection |
| Inflammation | Rheumatological disorder, inflammatory bowel disease |
| Smoking | See below |
| Metabolic syndrome | Diabetes, hypertension, obesity |
| Cushing’s | Suggestive history and physical exam |
| Solid tumor | Constitutional symptoms or symptoms referable to the involved organ(s) |
| Medication | Steroids, lithium or beta agonists |
| Stress | Emotional stress, extreme exercise |
| Splenectomy | Or hypospenism |
Diagnosis:
Diagnosis of exclusion
Diagnosis is supported by normalization of counts upon smoking cessation.
Smoking is associated with mild elevation of white cell count. If the white cell count/neutrophil count are greatly increased, other causes should be sought.
In a 2005 study of 784 smokers, the baseline parameters (before smoking cessation) were:
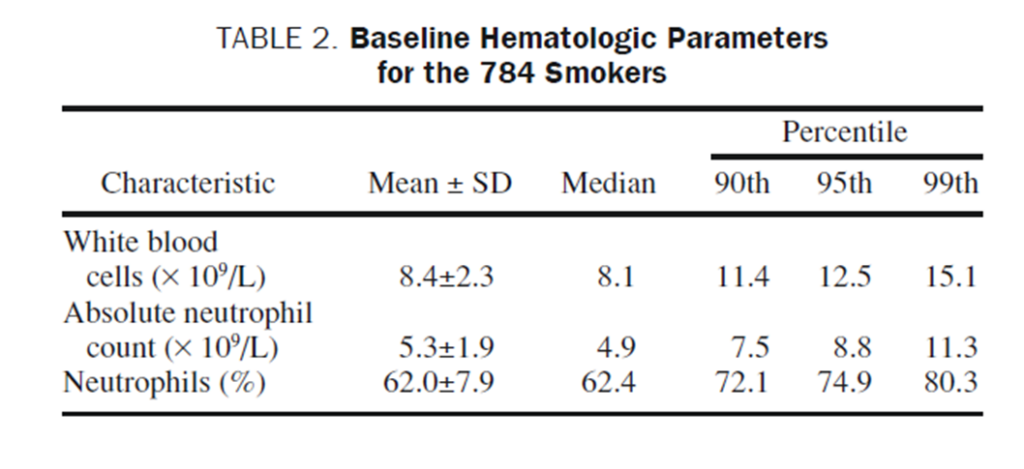
The authors wrote the following:
Should a smoker with a confirmed WBC count of 14.0 × 109/L on routine laboratory examination be evaluated further? This WBC count is between the 95th and 99th percentile for the healthy smokers in our study. In the absence of an obvious source of infection or inflammation, such a patient would likely warrant further work-up despite his or her smoking status. In contrast, a smoker with a WBC count of 12.4 × 109/L is within the statistically normal range of our subjects.
Others might use different thresholds for investigating a patient with leukocytosis who smokes. The important point here is that if the white cell count is much higher than 15 x 109/L, we should be looking for other causes.
A more recent study from 2021 of 40 patients determined to have smoking-induced leukocytosis showed the following baseline parameters:
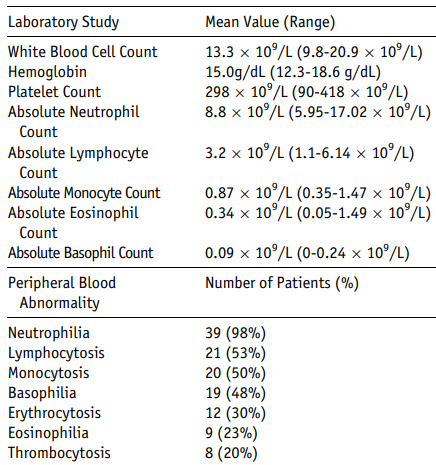
These authors concluded:
- Tobacco use leads to mild elevation of total white blood cell count.
- Associated primarily with neutrophilia, but also lymphocytosis, monocytosis, and basophilia.
- Tobacco history should be elicited from all patients presenting with leukocytosis to limit unnecessary diagnostic testing, and counseling regarding smoking cessation should be offered.
Treatment:
Smoking cessation!