Treatment
Clinical practice guideline recommendations for transfusion in vaso-occlusive crisis
NHLBI recommendations:

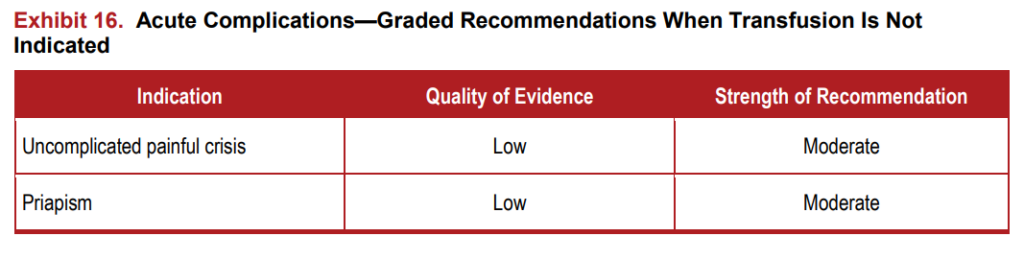

baseline value
British Society of Hematology recommendations:
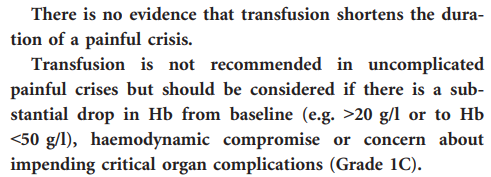
Bottom line:
Bottom line: do not routinely transfuse your patient with vaso-occlusive crisis… only if there is another indication to do so!
Course in hospital
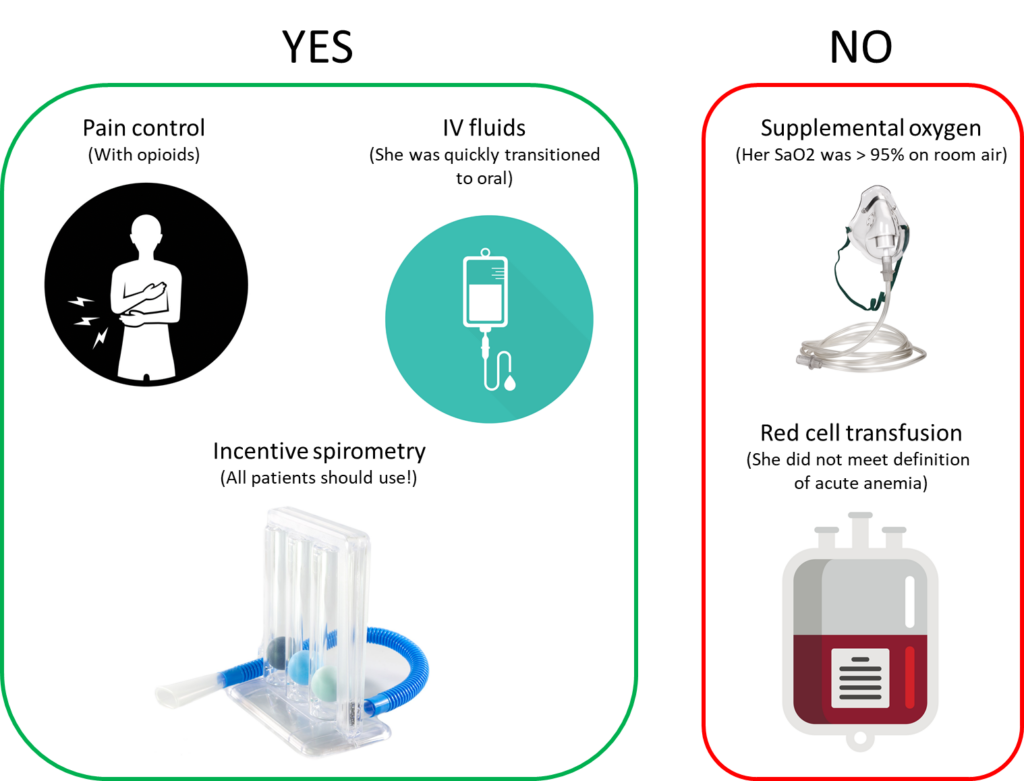
The patient was treated with opioids. Her oxygen saturations were consistently > 95%, so she did not require supplemental oxygen. She was instructed to use incentive spirometry every 4 hours while awake. She was initially started on IV fluids (normal saline) because she was in too much pain to take liquids orally, but she was transitioned to oral fluids shortly thereafter. She was not transfused with red cells. Her pain subsided over the next 5 days, and her hemoglobin increased to her baseline of about 8 g/dL. She was discharged from the hospital feeling fatigued, but otherwise well.
Schematic of what the patient received and did not receive: