Labs
The following results are from the complete blood count (CBC) the day you see the patient:
| WBC (109/L) | Hb (g/dL) | MCV (fL) | PLT (109/L) |
|---|---|---|---|
| 11.2 | 6.3 | 105 | 403 |
What’s what: WBC, white blood cell count; Hb, hemoglobin; MCV, mean cell volume; MCHC, mean cellular hemoglobin concentration; RDW-SD, red cell distribution width-standard deviation; platelets, PLT; Normal values: WBC 5-10 x 109/L, RBC 4-6 x 1012/L, Hb 12-16 g/dL, Hct 35-47%, MCV 80-100 fL, MCHC 32-36 g/dL, RDW-SD < 45 fL, platelets (PLT) 150-450 x 109/L
Indeed, the reticulocyte count was elevated:

Reticulocyte count is:
- 18.9% of the total red cell count
- 0.35 x 1012/L or 350 x 109/L
Focus on the absolute reticulocyte count. It keeps things simple. An absolute reticulocyte count >120 x 109/L is considered an appropriate response to anemia.
Therefore, this patient has a hyperproliferative anemia.
Here are data on baseline hemoglobin concentration (Hb) from a large series of patients with HbSS:

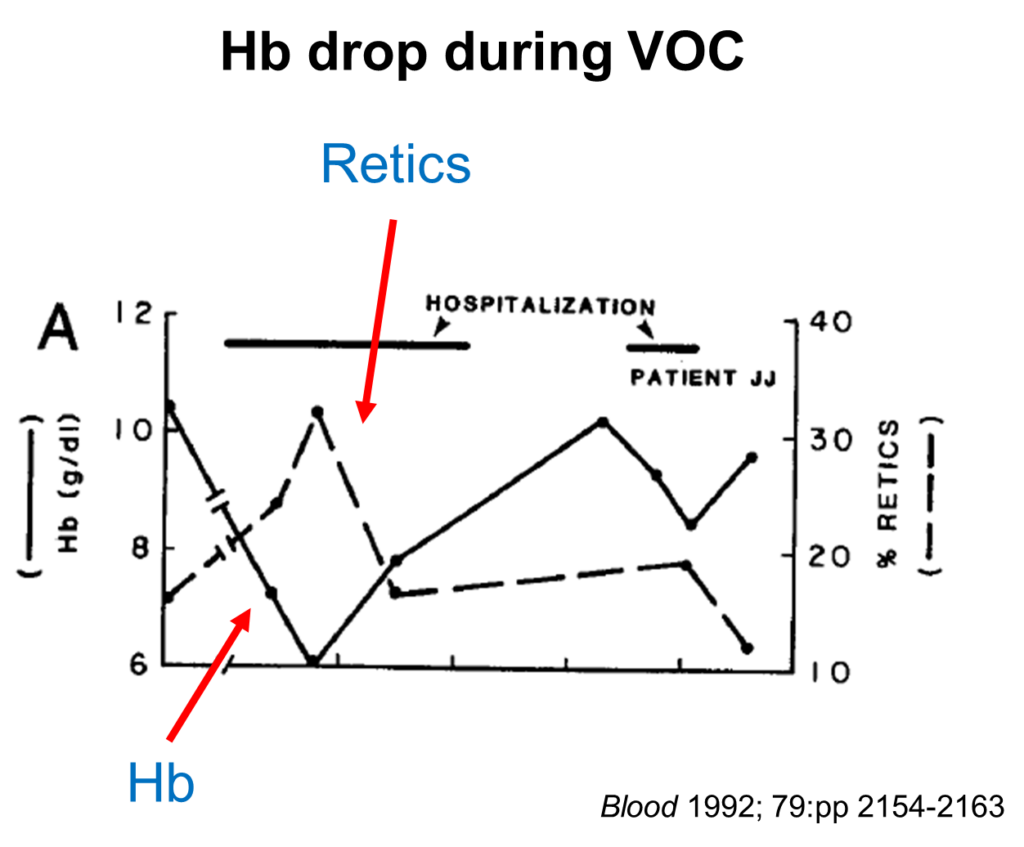
Most patients with a veno-occlusive crisis (VOC) experience a drop in hemoglobin (Hb) of 1-2 g/dL. Here is a nice example from a single patient during the course of their pain crisis (note how the drop in Hb is accompanied by an increase in % reticulocytes [% retics]):
The patient has a new (albeit mild) leukocytosis. This is not unusual in a case of vaso-occlusive crisis. Here is her white blood cell differential:
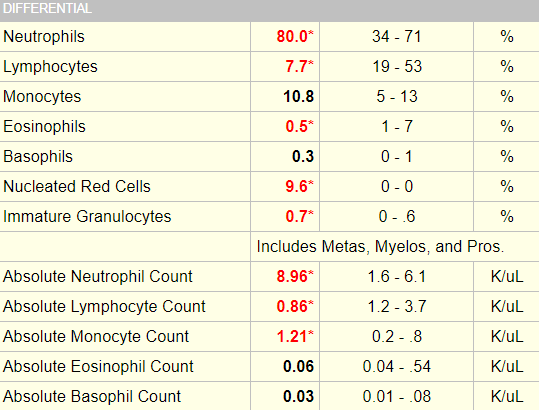

These data indicate neutrophilia, lymphopenia and monocytosis (remember, focus on the absolute counts). How can we make these determinations? By referring to our cheat sheet!
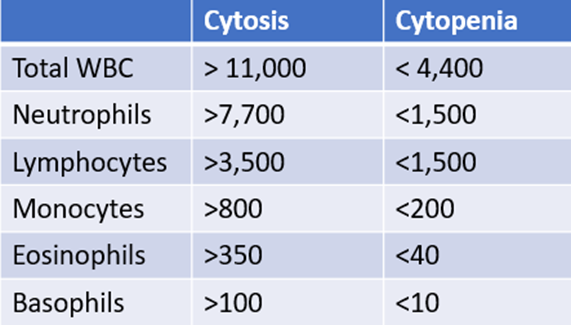
The patient’s white cell differential is consistent with stress.