Treatment

Is there anything to choose between prednisone 1 mg/kg and the 4-day dexamethasone regimen?
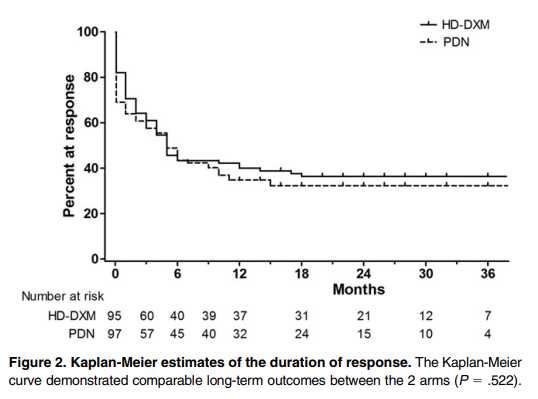
According to the 2019 ASH guideline, you might consider dexamethasone over prednisone if rapid initial platelet response is important. This recommendation is based on the results of a randomized trial comparing prednisone and dexamethasone showing shorter time to response in the dexamethasone arm. In a metanalysis of randomized trials comparing these two steroid regimens, platelet counts were higher at 14 days in patients receiving dexamethasone, but overall responses at 6 months did not differ significantly. Prednisone is associated with higher rates of weight gain and cushingoid appearance, whereas dexamethasone may be associated with higher rates of neuropsychiatric symptoms.
The following is a comparison between prednisone 1 mg/kg and the 4-day dexamethasone in treating newly diagnosed adult ITP:
| Parameter | Prednisone | Dexamethasone |
|---|---|---|
| Initial response rate | 60%-80% | 60-80% |
| Time to initial response | 4-14 days | 2-14 days |
| Time to peak response | 7-28 days | 4-28 days |
| Sustained response | 30%-50% | 30%-50% |
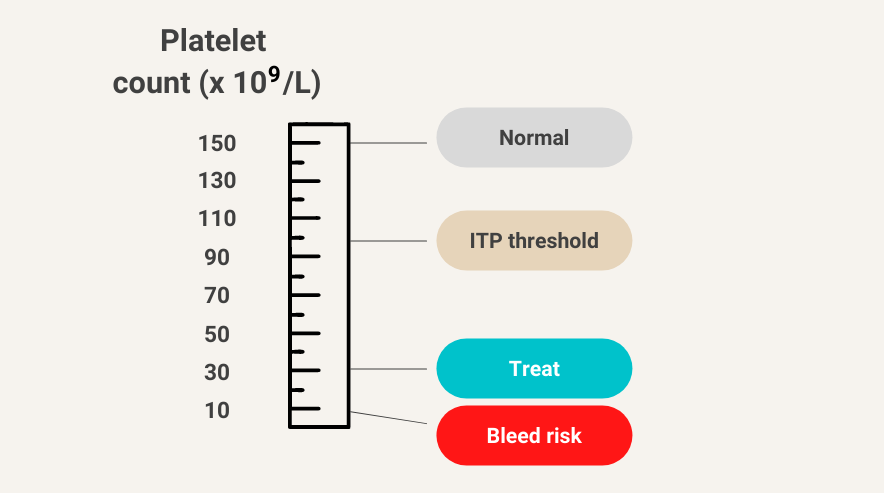
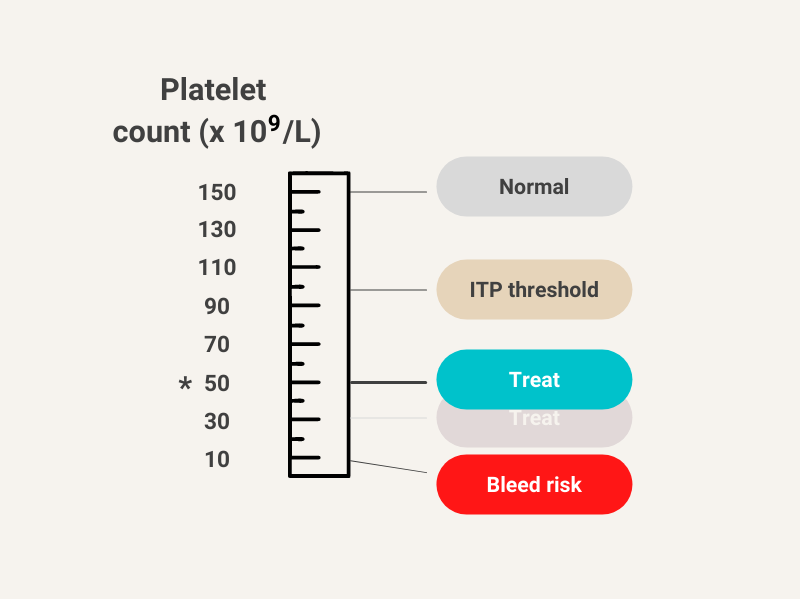
Spontaneous bleeding is uncommon at platelet counts >30 × 109/L