Labs
Here is the patient’s complete blood count (CBC) when you see him in clinic:
| WBC | Hb | Hct | MCV | MCHC | RDW-SD | PLT |
|---|---|---|---|---|---|---|
| 5.2 | 11.2 | 40 | 78 | 28 | 42 | 5 |
What’s what: WBC, white blood cell count; Hb, hemoglobin; MCV, mean cell volume; MCHC, mean cellular hemoglobin concentration; RDW-SD, red cell distribution width-standard deviation; platelets, PLT; Normal values: WBC 5-10 x 109/L, RBC 4-6 x 1012/L, Hb 12-16 g/dL, Hct 35-47%, MCV 80-100 fL, MCHC 32-36 g/dL, RDW-SD < 45%, platelets (PLT) 150-450 x 109/L
We established in the section on Differential Diagnosis that the three likeliest possibilities in this outpatient with severe thrombocytopenia and an unremarkable history include:
- Immune thrombocytopenia
- Pseudothrombocytopenia
- Familial (congenital) thrombocytopenia
The peripheral smear from our patient is shown here:
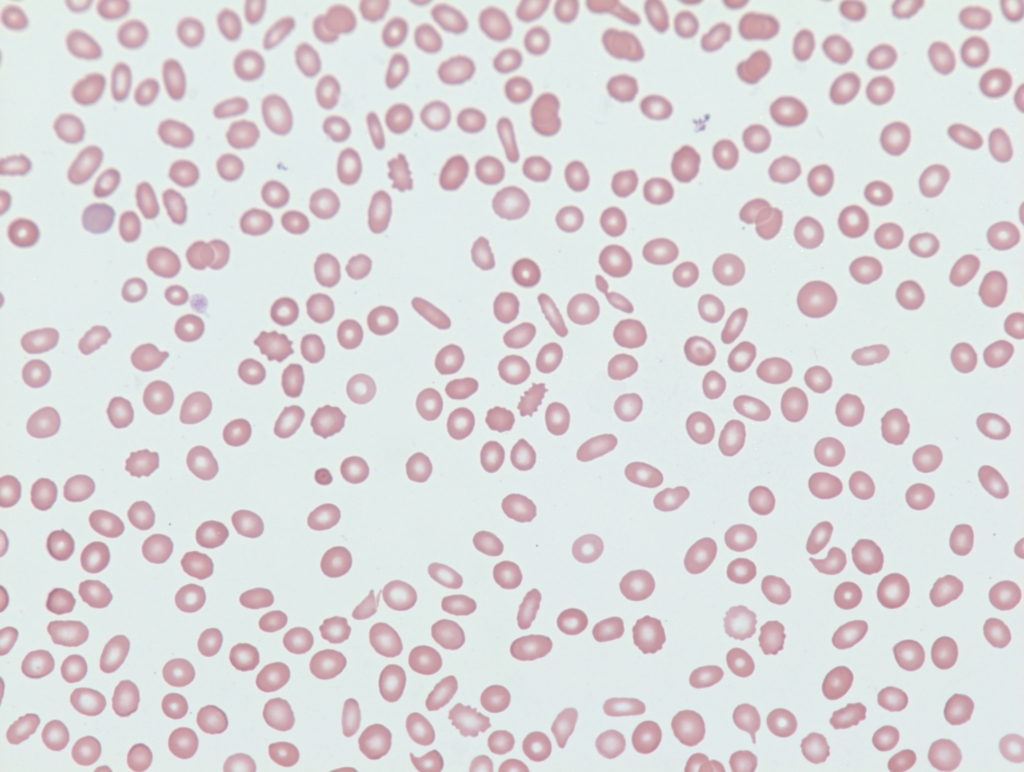
The patient is admitted directly to the hospital
