Labs and Course in Hospital
The following is the complete blood count (CBC) at the time of admission:
| WBC (109/L) | Hb (g/dL) | Hct (%) | MCV (fL) | RDW-SD (fL) | PLT (109/L) |
|---|---|---|---|---|---|
| 1.6 | 10.0 | 29 | 86 | 35.8 | 77 |
What’s what: WBC, white blood cell count; Hb, hemoglobin; MCV, mean cell volume; MCHC, mean cellular hemoglobin concentration; RDW-SD, red cell distribution width-standard deviation; platelets, PLT; Normal values: WBC 5-10 x 109/L, RBC 4-6 x 1012/L, Hb 12-16 g/dL, Hct 35-47%, MCV 80-100 fL, MCHC 32-36 g/dL, RDW-SD < 45 fL, platelets (PLT) 150-450 x 109/L
White blood cell differential:
| Cell type | Patient’s result |
|---|---|
| Neutrophil | 1.39 x 109/L |
| Lymphocyte | 0.14 x 109/L |
| Monocyte | 0.06 x 109/L |
| Eosinophil | 0.00 x 109/L |
| Basophil | 0.00 x 109/L |
In case you are not sure how to characterize white blood cell (WBC) subtype counts, here is a helpful cheat sheet!

Notice how elevated (cytosis) or reduced (cytopenia) counts of the 5 subtypes of white blood cells are defined by ABSOLUTE COUNTS, not percentages!!
For those who have the habit of examining the percentages, consider the following examples:
| Label | Total WBC (x 109/L) | Neutrophil % | ANC (x 109/L) | Lymphocyte % | Lymphocyte count (x 109/L |
|---|---|---|---|---|---|
| Normal | 10.0 | 60 | 6.0 | 20 | 2.0 |
| Patient 1 | 0.1 | 100 | 0.1 | 0 | 0 |
| Patient 2 | 200 | 2 | 4.0 | 80 | 160 |
Which the above case(s) is/are associated with neutropenia?
So, at this point we have a 44 year-old man with constitutional symptoms and pancytopenia.
The reticulocyte count was only 0.1 x 109/L. This is an inappropriate response to anemia.
The results of this patient’s acute phase response:
| Marker | Patient results (normal range) |
|---|---|
| Positive acute phase protein | |
| CRP | 40.7 (0-5 mg/L) |
| Fibrinogen | 230 (180-400 mg/dL) |
| Haptoglobin | <10 (30-200 mg/dL) |
| Negative acute phase protein | |
| Transferrin (TIBC) | 128 (200-360 mg/dL) |
| Albumin | 3.3 g/dL (3.5-5.2 g/dL) |
The elevated ferritin and CRP, and the low TIBC and albumin support the presence of inflammation. While haptoglobin is a positive acute phase reactant, it is highly sensitive to hemolysis and levels will be low when there is concomitant inflammation and hemolysis. The fibrinogen is inappropriately low relative to other acute phase proteins.
Note that an ESR was not obtained.
Based on the information so far, is there another diagnosis we should consider that was not included in our original differential diagnosis of pancytopenia?
At this point, the diagnosis of hemophagocytic lymphohistiocytosis (HLH) is on the table. Are you familiar with any diagnostic scoring system for HLH?
Let’s look at each scoring system in turn:
HLH-2004
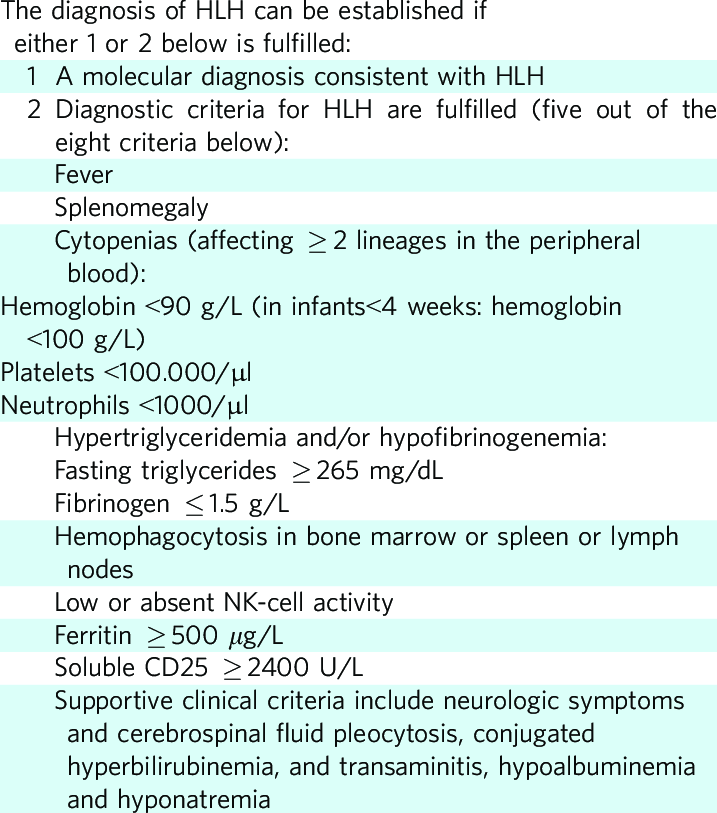
This patient met the following criteria:
- Fever
- Splenomegaly
- Cytopenias
- Increased triglycerides (results were 320 mg/dL)
- Increased ferritin
Note: sIL2R and pathology take several days to come back. But in this case, we have 5/8 criteria, suggestive of HLH.
HScore

The calculator for the HScore can be found here.
This patient’s score was 254 suggesting > 99% probability of HLH.
Scoring breakdown:
- Temperature > 102.9 (+49)
- Splenomegaly alone (+23)
- 3 lineagecytopenia (+34)
- Ferritin > 6,000 ng/mL (+50)
- Triglycerides 132.7-354 mg/dL (+44)
- Fibrinogen > 250 mg/dL (+0)
- AST > 30 U/L (+19)
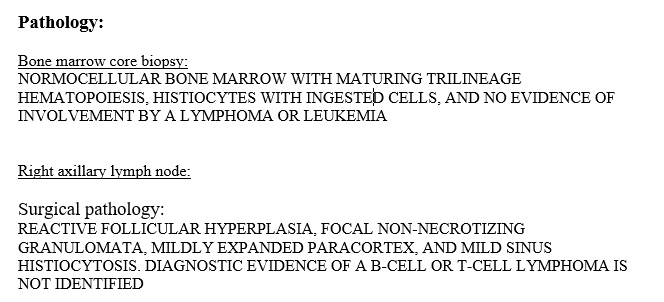
- Hemophagocytosis features on bone marrow aspirate (+35)
Given concern for an underlying malignancy as the driver of his pathologic condition, the patient undergoes an excisional biopsy of an enlarged right axillary lymph node. He subsequently undergoes PET-CT to evaluate for other areas of FDG uptake.
Why is fine needle aspiration (FNA) inadequate for the diagnosis of suspected lymphoma?
Click for AnswerFDG PET:CT – no abnormal FDG uptake identified
The soluble IL-2 receptor was 3131 pg/mL (normal range 175.3-858.2 pg/ml).