How expert consultants constrain probability, recalibrate posture, and make judgment visible when immune reserve is falling and danger is often hidden
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Neutropenia Is Not Just a Count
It is a reserve-threat signal.
New-onset neutropenia in a hospitalized patient is not primarily a diagnostic problem.
It is a vulnerability problem.
The absolute neutrophil count does not simply describe marrow output.
It signals shrinking immune reserve, muted warning signs, and asymmetric risk.
The same ANC can live in very different clinical worlds:
• expected treatment-related suppression
• hidden infection risk with preserved stability
• evolving marrow failure
• overlapping medication and inflammatory effects
• catastrophic reserve loss with rapid deterioration
In each case, the number may look similar.
The danger is not.
This is why hospital neutropenia is not managed safely by diagnosis alone.
It is managed by posture.
Consult Practice makes that posture explicit.
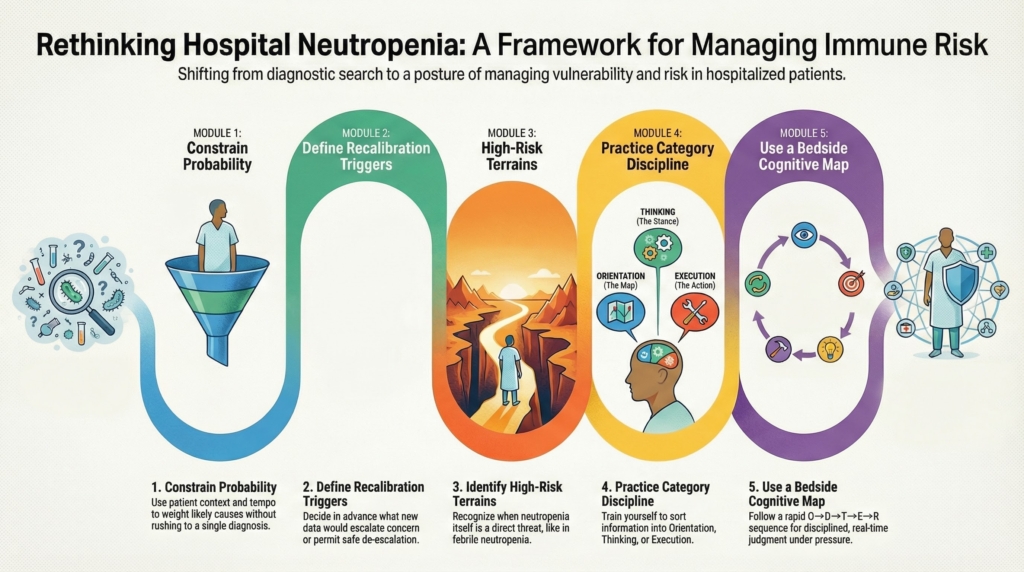
The Five-Module Framework for Neutropenia
This series uses five applied modules to teach how expert consultants manage neutropenia as a reserve-threat pattern, not just a laboratory abnormality.
Each module performs a different cognitive function:
Module 1 — Most Likely in This Context
Early weighting by terrain and tempo
Constrains probability without naming a diagnosis.
It answers:
Given this inpatient setting, trajectory, and severity, what functional explanations deserve the most weight right now?
This module teaches how context and tempo narrow the probability space before unification is earned.
Module 2 — What Would Change the Posture
Trajectory- and trigger-based reassessment
Defines what new data should escalate concern, justify continued vigilance, or permit safe release.
It answers:
What would make me think differently in six hours or tomorrow?
This module makes recalibration explicit and protects against both premature reassurance and unnecessary escalation.
Module 3 — Disease-Specific Applied Danger Frame
When neutropenia becomes dangerous in itself
Highlights rare but high-risk terrains where neutropenia is not just a signal, but a direct threat.
For neutropenia, this includes patterns such as:
• febrile neutropenia as a reserve-threat terrain
• rapid marrow suppression with systemic vulnerability
• contexts where muted signs hide escalating danger
It answers:
When does this abnormality demand immediate protective posture regardless of cause?
Module 4 — Boundary Drill (Practice & Reflection)
Orientation vs Thinking vs Execution
Trains category discipline.
Learners practice sorting information into:
• terrain definition (Orientation)
• stance and weighting (Thinking)
• visible behavior and communication (Execution)
It answers:
Am I defining the map, assigning weight, or directing action?
This module prevents lens drift and teaches posture explicitly.
Module 5 — Quick-Access Card
Compressed bedside cognitive map
Provides rapid posture reminders under pressure.
It answers:
What stance should I adopt right now?
This module reinforces the O → D → T → E → R cognitive sequence and supports real-time consult judgment without becoming an algorithm.
Why This Modular Approach Matters
Most errors in hospital neutropenia do not arise from missing rare diagnoses.
They arise from:
• underestimating reserve loss
• anchoring on “expected” suppression too early
• allowing muted signs to lower vigilance
• failing to revise posture as trajectory evolves
• confusing explanation with danger management
This modular system protects against those failures by:
• constraining probability before unification
• making recalibration an expected discipline
• preserving vigilance for rare but catastrophic terrain
• enforcing category discipline
• supporting rapid bedside posture under pressure
How to Use This Series
Start with Module 1 to constrain probability by context and tempo.
Use Module 2 to recalibrate as new data appear.
Consult Module 3 when neutropenia itself becomes a danger terrain.
Train with Module 4 to strengthen lens discipline.
Rely on Module 5 for rapid bedside posture.
These modules are designed to be used together.
Not as algorithms.
Not as cause lists.
But as a method for managing shrinking immune reserve safely in real clinical time.
Bottom Line
Hospital neutropenia is not a diagnosis.
It is a reserve-threat signal.
Expert care depends on:
• constraining probability by terrain
• revising posture by trajectory
• preserving vigilance for hidden danger
• and making judgment visible as biology evolves
That is how expert consultants manage neutropenia when immune reserve is falling and the stakes are real.