What bothers us may reveal more about how we listen than how trainees speak.
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
On rounds, these moments arrive quietly.
A hand gesture. A compressed sentence. A pause that only the listener feels.
Acronyms that multiply faster than they clarify.
Sentence fragments delivered like headlines.
“Status post,” that elastic phrase that stretches across time without saying where it begins or ends.
Hands that point as if the body were a diagram.
Fillers that ripple through a presentation, like static between stations.
None of these prevent understanding.
The story is there.
The physiology is intact.
The reasoning often holds.
And yet something in me notices.
The Question Beneath the Reaction
For years I assumed the noticing meant something was wrong with the speaker.
Lately I wonder if it is telling me something about the listener.
Why does this bother me?
Loss of rigor?
Loss of form?
Loss of something harder to name?
Or simply that I learned to listen in a different linguistic world?
Irritation, it turns out, is not a conclusion.
It is a clue.
Two Grammars of Medicine
Every generation inherits a speech culture along with its textbooks.
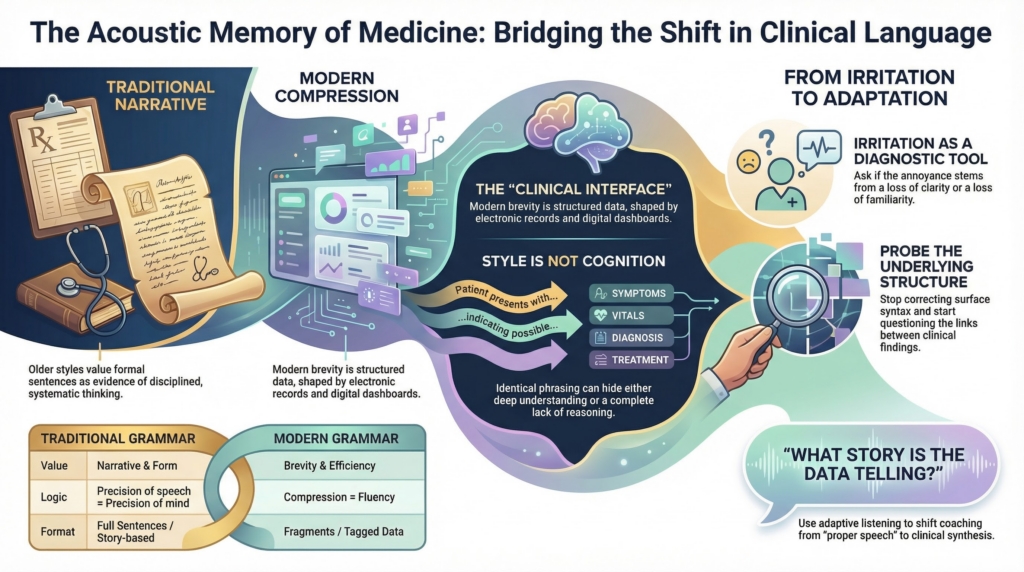
In the environments where many of us trained, language carried moral weight. Full sentences signaled discipline. Formal phrasing signaled seriousness. Precision of speech suggested precision of mind. The case presentation was not merely informational. It was performative evidence of thought.
Today’s trainees were shaped inside a different linguistic climate. Their professional language matured alongside templated notes, electronic records, dashboards, and compressed digital communication. Information is packaged, tagged, abbreviated, transmitted. Brevity is fluency. Compression is efficiency.
Seen from that angle, the fragmentary physical exam is not broken speech. It is structured data delivered orally.
“S1 S2 no murmurs, lungs clear, abdomen soft nontender” is not linguistic erosion.
It is a clinical interface.
What Actually Matters
Style is not the same as cognition.
Some linguistic habits genuinely shape thinking. Language that blurs distinctions can blur reasoning. Overloaded acronyms can collapse important differences. Vague temporal phrases can obscure trajectory. When language hides structure, thought can follow.
But here is the harder truth.
At the bedside, you often cannot tell.
One trainee says,
“status post surgery,”
and cannot say when, which surgery, or what changed afterward.
Another says the exact same words
and can immediately specify the procedure, the timeline, and its clinical relevance.
The problem is not that the phrase is abbreviated. The problem is that it sounds complete while leaving the clinical state undefined. “Status post” reports that something happened. It does not tell you what it did. Did the patient improve, worsen, return to baseline, develop a complication, or acquire a new risk? Chronology is supplied. Physiology is not.
The surface is identical.
The cognition is not.
The real pedagogical difficulty is not deciding which linguistic habits matter.
It is recognizing, in real time, that compressed language alone cannot tell you which is which.
Sentence fragments can conceal thought.
Sentence fragments can also transmit it perfectly.
The ear cannot reliably tell which one it hears.
The Suspicion
What unsettles us is often not loss of clarity.
It is loss of familiarity.
Every profession has an acoustic memory, a remembered sound of what competence used to sound like. When that sound changes, we feel the shift before we understand it. Difference can register as decline simply because it is new.
The ear is conservative.
Language evolves anyway.
What Might Actually Be Changing
It is possible something is being lost.
Older presentation styles did more than sound formal. They forced narration. To describe a finding in a full sentence is to place it inside a story. Subject. Verb. Interpretation. Connection. The grammar itself nudges the mind toward synthesis.
Fragmented delivery does not always demand that same integration. It can transmit data without obligating narrative. That is not necessarily worse. But it is different.
If something cognitive is lost when narration disappears, the task is not to resurrect an old style.
It is to replace the cognitive work that style once required.
Irritation as Data
It is tempting, in these moments, to correct the speaker. Sometimes correction is warranted. Language should be coached when it obscures reasoning or hides uncertainty.
But just as often, the more interesting move is inward.
Why did that phrase catch me?
What did I expect to hear instead?
Is my concern about clarity of thought
or allegiance to a vanished sound?
Our irritations on rounds can function as diagnostic instruments. Not of trainees, but of ourselves. They reveal our assumptions about what language is for, what professionalism sounds like, and how closely speech must resemble the forms that once taught us how to think.
I am beginning to test myself in these moments. Did I lose the reasoning, or did I just dislike the phrasing? The answer determines what happens next. Sometimes I ask for clarification. Sometimes I ask for the story. And sometimes I simply listen longer.
What Adaptation Looks Like
Adaptation does not mean lowering standards.
It means listening differently.
It sounds like:
Tell me how you’re linking those findings.
What story do you think the data are telling?
Which piece matters most to you?
Not:
Say that again properly.
Adapted listening shifts coaching from surface form to underlying structure. It stops correcting sentences and starts probing reasoning.
What the Listener Learns
The student at the bedside does not know any of this is happening. They are simply trying to tell the story clearly enough that the team can act. If the physiology is right, the reasoning sound, and the plan coherent, communication has succeeded, even if the sentences never quite assembled themselves along the way.
The deeper discipline for those of us listening is to distinguish between language that fails thought and language that merely fails our expectations.
Only one requires correction.
The other requires adaptation.