Vitamin K antagonists disrupt the carboxylation of vitamin K-dependent coagulation factors (factors II, VII, IX, and X; and protein C and protein S). Administration of vitamin K restores hepatic carboxylation of the vitamin K-dependent coagulation factors in a dose-dependent manner. Since this requires new protein synthesis, administration of vitamin K does not result in immediate correction of coagulopathy. 12-24 hours are required for a sufficient amount of newly synthesized carboxylated vitamin K-dependent coagulation factors to reconstitute hemostasis.
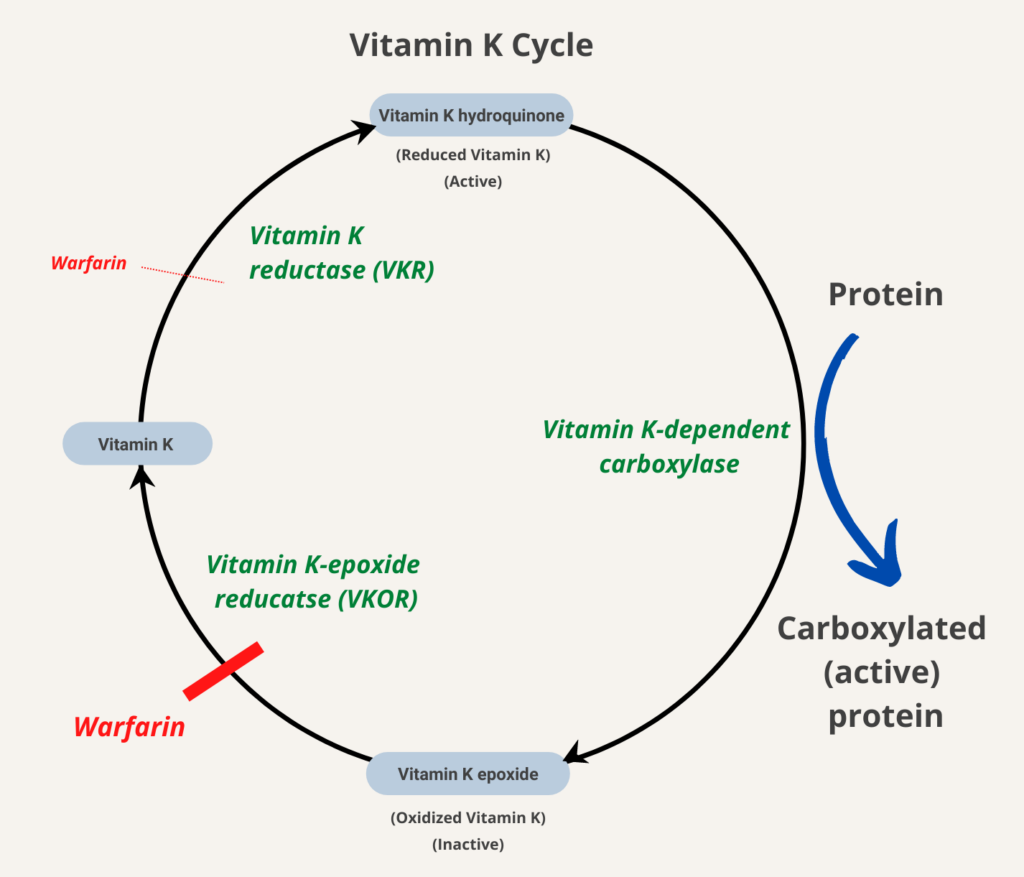
The enzyme that modifies the vitamin K-dependent proteins such as factors II, VII, IX and X, is the vitamin K-dependent carboxylase (or vitamin K-dependent gamma glutamyl carboxylase [GGCX]). This enzymes results in the carboxylation of of Glu to Gla residues. Concomitant with this modification, a reduced vitamin K molecule is converted to vitamin K epoxide. Before it can be reused, this vitamin K epoxide must be converted back to reduced vitamin K by the vitamin K epoxide reductase (VKOR). It is not known whether the conversion of vitamin K to reduced vitamin K is accomplished by VKOR or a separate enzyme. Thus, the unidentified reductase is referred to simply as vitamin K reductase (VKR) or vitamin K quinone reductase. Warfarin inhibits vitamin K epoxide reductase complex subunit 1 (VKORC1), thereby dampening the carboxylation and the procoagulant potential of vitamin K–dependent coagulation factor. To the extent that VKOR contributes to the conversion of vitamin K to reduced vitamin K, warfarin inhibits both reduction steps (indicated by red line).