Suspect diagnosis
- Suspect diagnosis of immune (acquired) TTP in adults with:
- Microangiopathic hemolytic anemia (MAHA)
- Thrombocytopenia
- New focal neurological findings
- Prior history of TTP
- Suspect diagnosis of congenital TTP in:
- Neonates with:
- Severe jaundice
- Microangiopathic hemolytic anemia
- Thrombocytopenia
- Children or adults with unexplained thrombocytopenia or a family history of TTP
- Pregnant adults with a first episode of TTP
- Neonates with:
Confirm diagnosis
- For immune TTP, diagnosis is confirmed by demonstrating reduced plasma ADAMTS13 activity (<10%) and the presence of a functional inhibitor of ADAMTS13 in mixing studies or anti-ADAMTS13 IgG antibodies.
- For congenital TTP, the following confirms the diagnosis:
- Reduced plasma ADAMTS13 activity (<10%)
- Absence of anti-ADAMTS13 antibodies
- Presence of a homozygous or compound heterozygous ADAMTS13 variant in genetic screening
Clinical scoring systems
- ADAMTS13 activity levels take several days to come back.
- Thus, conditional diagnosis (to initiate appropriate treatment) is based on point-based clinical scoring systems (also referred to as clinical prediction rules, pretest probability tools), which predict the probability of severely deficient ADAMTS13 activity levels.1
- Importantly, these scores are not meant to replace ADAMTS13 testing but to aid decision making until test results are available.
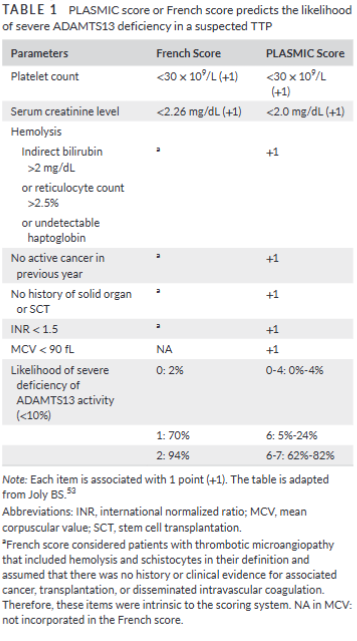
- There are two validated clinical prediction rules:

in suspected TTP. Source.
Order set in patient with suspected TTP
| Parameter | Typical Result(s) |
|---|---|
| CBC | Anemia, thrombocytopenia |
| Peripheral smear | Schistocytes, polychromatophilia |
| Reticulocyte count | Elevated |
| Haptoglobin | Low |
| LDH | Elevated2 |
| Indirect bilirubin | Elevated |
| Creatinine | Normal3 |
| Troponin T | May be elevated |
| Liver function tests | Normal |
| PT/aPTT | Normal |
| Coombs test | Negative |
| ADAMTS13 activity | <10% |
ADAMTS13 assays
- Use pretreatment blood samples to determine ADAMTS13 activity level and to test for anti-ADAMTS13 antibodies.
- ADAMTS13 activity:
- Severe ADAMTS13 deficiency, which is defined by an activity level <10%, is required to confirm the diagnosis of TTP.
- ADAMTS13 activity assays are based on degradation of either full-length VWF or synthetic peptides of VWF by ADAMTS13 in the plasma sample being tested.4
- ADAMTS13 activity testing is labor intensive, time consuming, and typically limited to reference laboratories.5
- VWF cleavage products are detected by:
- Fluorescence resonance energy transfer (FRET)-based assays (the method of choice in many institutions)6
- Enzyme-linked immunosorbent assay (ELISA)
- Surface-enhanced laser desorption/ionization time-of-flight mass spectrometry (SELDI-TOF)
- Fully automated chemiluminescence-based assays and semiquantitative point-of-care assays are now also available, but inconsistencies have been reported between different testing platforms.
- Testing for anti-ADAMTS13 autoantibodies:
- When severely deficient ADAMTS13 activity is confirmed, the next step of investigation is to determine if an antibody inhibitor to ADAMTS13 is present.7
- Critical in differentiating immune TTP from congenital TTP.8
- Most anti-ADAMTS13 autoantibodies are of the IgG isotype (IgG4 is most common, followed by IgG1) but IgM and IgA isotypes have also been identified.
- Anti-ADAMS13 antibodies are measured using one of the following methods:
- Enzyme-linked immunosorbent assay (ELISA)
- Western blot
- Immunoprecipitation
- ADAMTS13 antigen can be measured by ELISA but this is not yet part of routine clinical practice.9
What the clinical practice guidelines say
- International Society on Thrombosis and Haemostasis (ISTH) guideline on the diagnosis of thrombotic thrombocytopenic purpura:
- In settings with timely access to plasma ADAMTS13 activity testing and for patients with a high clinical suspicion (≥90% pretest probability) of immune TTP (e.g., based on clinical assessment or a formal clinical risk assessment method), the panel suggests the following diagnostic strategy. (A conditional recommendation in the context of low certainty evidence.):
- Step 1: Acquire a plasma sample for ADAMTS13 testing (e.g., ADAMTS13 activity and inhibitors or anti-ADAMTS13 IgG) before an initiation of TPE or use of any blood product.
- Step 2: Start TPE and corticosteroids without waiting for the results of ADAMTS13 testing.
- Step 3: Consider early administration of caplacizumab before receiving plasma ADAMTS13 activity results.
- Step 4: When the result of plasma ADAMTS13 activity is available, continue caplacizumab if ADAMTS13 activity is less than 10 IU/dL (or <10% of normal) (a positive result) or stop caplacizumab and consider other diagnoses if ADAMTS13 activity is >20 IU/dL (or >20% of normal) (a negative result).
- Step 5: For patients with plasma ADAMTS13 activity less than 10 IU/dL (or <10% of normal) (a positive result), also consider adding rituximab as early as possible, as a majority of these adult patients (>95%) have autoantibodies against ADAMTS13.
- In settings with a timely access to plasma ADAMTS13 testing and for patients with intermediate or low clinical suspicion of immune TTP (e.g., based on clinical assessment or a formal clinical risk assessment method), the panel suggests the following diagnostic strategy. (A conditional recommendation in the context of low certainty evidence.):
- Step 1: Acquire a plasma sample for ADAMTS13 testing (eg, ADAMTS13 activity and inhibitor or anti-ADAMTS13 IgG) before an initiation of TPE or use of any blood product.
- Step 2: Consider starting TPE and corticosteroids, depending on the clinician’s judgment and assessment of the individual patient.
- Step 3: Do not start caplacizumab until the result of plasma ADAMTS13 activity becomes available.
- Step 4: When the result of plasma ADAMTS13 activity testing is available, consider adding caplacizumab and rituximab (see Recommendation 2 in Treatment Guidelines) if ADAMTS13 activity is less than 10 IU/dL (or <10% of normal) with inhibitors or an elevated level of anti-ADAMTS13 IgG (a positive test result), but do not start caplacizumab and consider other diagnoses if ADAMTS13 activity is greater than 20 IU/dL (or >20% of normal) (a negative result).
- In settings with timely access to plasma ADAMTS13 activity testing and for patients with a high clinical suspicion (≥90% pretest probability) of immune TTP (e.g., based on clinical assessment or a formal clinical risk assessment method), the panel suggests the following diagnostic strategy. (A conditional recommendation in the context of low certainty evidence.):
- British Society for Haematology (BSH) guideline on the diagnosis and management of thrombotic thrombocytopenic purpura and thrombotic microangiopathies:
- International consensus defines TTP as MAHA with moderate or severe thrombocytopenia, with associated organ dysfunction—this can include neurological, cardiac, gastrointestinal and renal involvement. The presence of specific organ dysfunction is not a prerequisite for diagnosis, which is confirmed by demonstrating a severe deficiency of ADAMTS13 (<10 IU/dL).
- TTP remains a diagnosis suspected from the clinical history, examination and laboratory parameters including the blood film to aid exclusion of other TMAs. Assays for ADAMTS13 help to confirm the diagnosis and monitor the course of the disease and requirement for additional treatments.
- Tests include:


- British Society for Haematology (BSH) guideline (cont’d)
- Recommendations:
- The initial diagnosis of TTP and treatment decisions should be made on clinical history, examination and laboratory testing including blood film. (1A)
- Pretreatment samples should be obtained to measure ADAMTS13 activity levels and to detect anti-ADAMTS13 antibodies. (1A)
- The early measurement of ADAMTS13 activity is recommended over using scoring systems. (2C)
- Serological tests for HIV, HBV and HCV, autoantibody screen and when appropriate, a pregnancy test, should be performed at presentation. (1A)
- A low ADAMTS13 activity level based on a fully automated assay/semi-quantitative assay may require confirmation (by a FRETS-based assay) depending on the index of clinical suspicion for TTP. (2C)
- British Society for Haematology (BSH) levels of evidence and strength of recommendations based on Grading of Recommendations Assessment, Development and Evaluation (GRADE):
- Strength of recommendation
- Grade 1 – strong recommendation, benefits do, or do not, outweigh risks and burdens; applied to most patients with words such as “recommend”, “offer” and “should”
- Grade 2 – weak recommendation, benefits, risks, and burdens finely balanced, or appreciable uncertainty exists about magnitude of benefits and risks; consider patient values and preferences; use words such as “suggest”, “consider”
- Quality of evidence:
- Level A (high) – further research very unlikely to change confidence in estimate of effect
- Level B (moderate) – further research likely to have important impact on confidence in estimate of effect, may change estimate
- Level C (low) – further research very likely to have important impact on confidence in estimate of effect and likely to change estimate
- Level D (very low) – any estimate of effect is very uncertain
- Strength of recommendation
- Recommendations:
Want to explore this further?
Check out the related sections in our TTP module:
- TTP – Plasmic Score
- Video Lecture on TTP Diagnosis
- TTP Clinical Presentation – Quiz