Clinical presentation
Clinical presentation of TTP is highly variable, ranging from minimal symptoms to critical illness, but typically includes a combination of:
- Microangiopathic hemolytic anemia (MAHA) (median hemoglobin 8-10 g/dL)
- Thrombocytopenia (median platelet count 10-30 × 109/L)
- Organ dysfunction
The historic pentad is present in only 5% of patients, and includes:1
- Thrombocytopenia
- Microangiopathic hemolytic anemia
- Neurologic symptoms
- Kidney impairment
- Fever
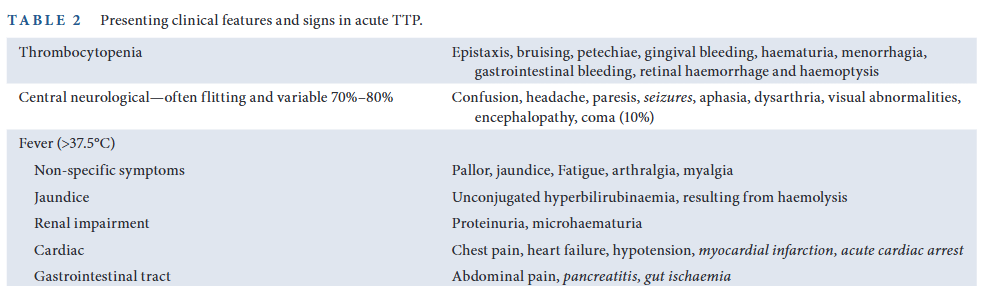
Symptoms
Symptoms may include those of:
- Anemia:
- Weakness
- Fatigue
- Jaundice
- Pallor
- Thrombocytopenia:
- Petechiae/purpura
- Bleeding, for example:
- Epistaxis
- Gingival bleeding
- Gastrointestinal bleeding
- Hematuria
- Menorrhagia
- Hemoptysis
- Retinal hemorrhage
- Organ dysfunction, including:2
- Neurologic (about 60% of cases), including:3
- Confusion
- Headaches
- Stroke
- Coma
- Seizures
- Visual changes
- Altered speech
- Paresthesia
- Cardiovascular (heart ischemia in about 25% of cases), including:4
- Chest pain
- Arrhythmias
- Symptoms of heart failure, for example:
- Paroxysmal nocturnal dyspnea
- Orthopnea
- Dyspnea on exertion
- Fatigue and weight gain
- Cough
- Hypotension
- Myocardial infarction
- Acute cardiac arrest
- The gastrointestinal tract:
- Mesenteric ischemia (about 35% of cases), which may present with:
- Abdominal pain
- Nausea
- Vomiting
- Diarrhea
- Patients may also present with pancreatitis1
- Mesenteric ischemia (about 35% of cases), which may present with:
- The kidney:
- Hematuria and proteinuria
- Rena failure rare
- Neurologic (about 60% of cases), including:3
- Conditions associated with secondary acquired/immune TTP such as those related to:
- Autoimmune diseases, especially SLE
- Pregnancy
- Drugs
- HIV infection
- Pancreatitis
- Cancer
- Organ transplantation
- Consensus on the standardization of terminology in thrombotic thrombocytopenic purpura and related thrombotic microangiopathies: “Acute TTP presentations may include bleeding symptoms such as bruising or hematuria, or thrombotic symptoms associated with neurologic or cardiac involvement.”5
Physical findings
- Look for:
- Vitals:
- Fever
- Hypotension
- Skin:
- Petechiae
- Echymoses
- Jaundice from hemolysis
- Pallor
- Neurological:
- Confusion
- Paresthesia
- Paresis
- Aphasia or dysarthria
- Visual changes
- Seizures
- Encephalopathy
- Fluctuating levels or consciousness
- Coma, which has been reported in 10% of patients with acute TTP
- Vitals:
Lab tests
- Thrombocytopenia:6
- Caused by consumption of platelets in platelet-rich thrombi.
- Median platelet count typically 10–30 × 109/L at presentation.
- MAHA:7
- Caused by mechanical fragmentation of erythrocytes during flow through partially occluded, high-shear small vessels.
- Median hemoglobin levels on admission are typically 8-10 g/dL.
- Evidence of hemolysis:
- Elevated LDH, caused by:
- Hemolysis
- Tissue ischemia
- Low haptoglobin
- Increased indirect bilirubin
- Elevated LDH, caused by:
- Evidence of schistocytes on peripheral smear
- PT, aPTT are typically normal.
- Elevated troponin levels (>50% of cases).
- Consensus on the standardization of terminology in thrombotic thrombocytopenic purpura and related thrombotic microangiopathies: “Anemia may not be immediately obvious. Thrombocytopenia is generally severe (platelet count of < 30 × 109/L), but higher platelet numbers do not exclude the diagnosis”.8
Cohort studies
- Scully et al, 2019
- 145 patients with TTP (ADAMTS13 activity at baseline was below 10% in 123 patients [85%])
- Median platelet count (range) – 24 × 109/L (3 × 109/L – 133 × 109/L)
- Median LDH (range) – 422 (120-3343)
- Page et al, 2017
- 78 patients with TTP (defined as ADAMTS13 activity <10%)
- Fever in 10% of patients
- Neurologic changes:
- Severe in 53% of patients
- Mild in 27%
- None in 20%
- Thrombocytopenia in100%:
- Median platelet count 10,000
- Platelet count:
- > 20 × 109/L in 14%
- > 30 × 109/L in 4%
- MAHA 100%:
- Median Hct 21%
- Hct >30 in 3%
- Only 14% of patients had serum creatinine concentrations ≥2.5 mg/dL
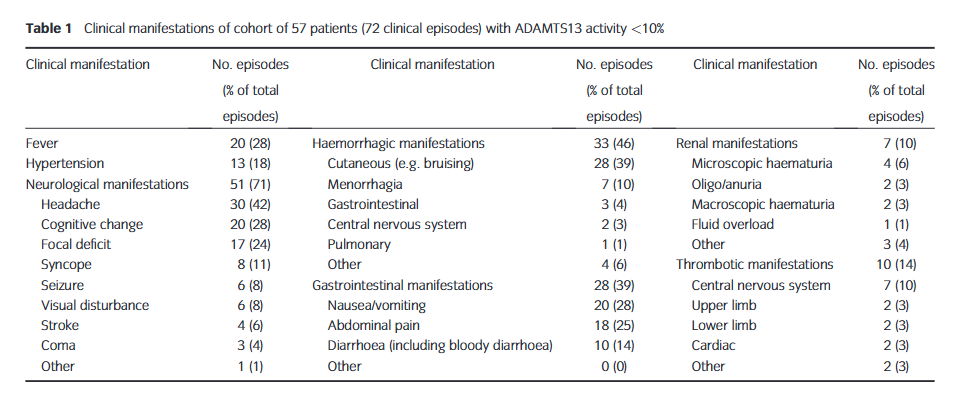
- Blombery et al, 2016
- 57 patients with TTP (defined as ADAMTS13 activity <10%), accounting for 72 episodes
- Neurological manifestations in 71% of episodes
- Hemorrhagic manifestations in 46% of episodes
- GI manifestations in 39% of episodes
- Fever in 28% of episodes
- Renal manifestations in 10% of episodes
- TTP pentad in 7% of episodes
Clinical practice guidelines
- A British Society for Haematology Guideline: Diagnosis and management of thrombotic thrombocytopenic purpura and thrombotic microangiopathies.
Want to explore this further?
Check out the related sections in our TTP module:
- TTP – History
- TTP – Physical examination
- TTP Clinical Presentation – Quiz