The hidden judgment of delegating to trainees
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Delegation sounds simple.
Give the trainee a task.
They do the work.
You supervise.
In practice, delegation is one of the hardest cognitive acts in consult medicine.
Because responsibility does not delegate cleanly.
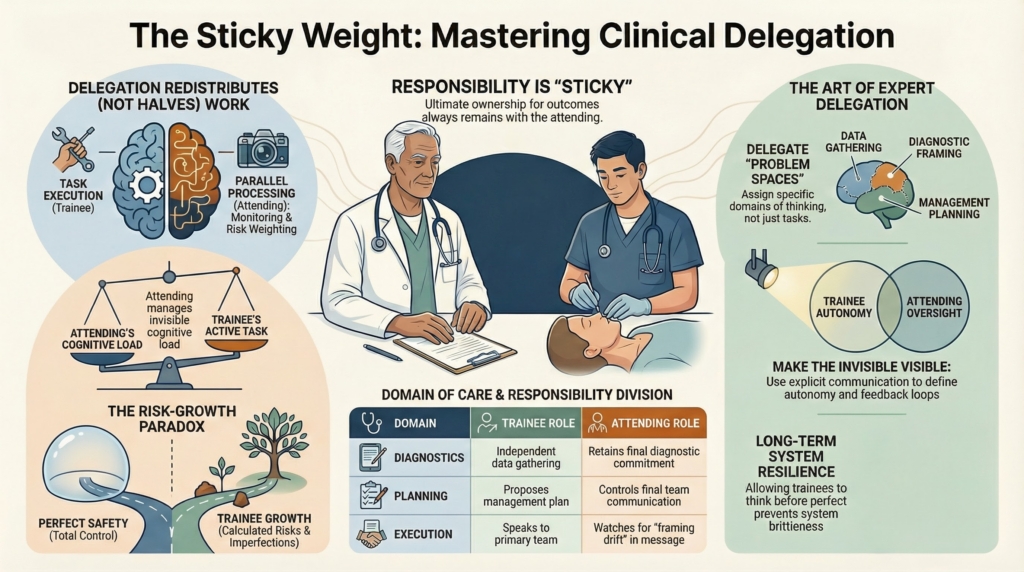
Responsibility is sticky
Even when a trainee is capable, the attending remains accountable.
For the decision.
For the outcome.
For the story told afterward.
This creates a structural tension.
You can give away tasks.
You cannot give away ownership.
The mind never fully lets go.
The invisible monitoring
When you delegate, you do not stop thinking.
You monitor.
You wonder:
Did they frame it the same way I would?
Did they ask the right questions?
Did they hear the same signal?
Did they weight the same risks?
Delegation becomes parallel processing.
You are both working.
One visibly.
The other silently.
Delegation does not halve cognitive work.
It redistributes it.
And it makes part of it invisible.
The fear of downstream surprise
Every attending knows the moment of downstream surprise.
You open the chart and see:
A note that misses the point.
A plan that sounds reasonable but is subtly wrong.
A call that went out with misplaced confidence.
The fear is not of error alone.
It is of surprise.
Of discovering that the trainee’s mental model
was not the one you thought they had.
Because you cannot directly inspect someone else’s thinking.
You infer it from fragments:
A note
A question
A presentation
A tone
Delegation is always an epistemic wager
on a mind you cannot fully see.
The tradeoff between safety and growth
Perfect safety requires control.
Perfect growth requires risk.
There is no version of delegation that gives you both fully.
Every attending is constantly balancing:
How much can I safely let go?
How much do they need to do themselves?
What kind of mistake is tolerable here?
These are not technical questions.
They are rarely named.
The distortion of hindsight
When things go well, delegation feels easy.
When things go badly, delegation is reinterpreted.
You should have checked.
You should have been more explicit.
You should have stepped in sooner.
Hindsight makes delegation look irresponsible.
In real time, it looked reasonable.
Institutions rarely punish over-supervision.
They frequently punish visible autonomy.
No one is reviewed for the trainee who never learned to think.
People are reviewed for the trainee who erred while learning.
The incentive structure is asymmetric.
So control feels safer than growth.
The trainee’s parallel experience
Trainees experience delegation differently.
They experience:
being trusted
being tested
being exposed
They see autonomy in what they are allowed to do.
They do not see the attending’s internal monitoring.
They do not see the parallel responsibility being carried above them.
So they interpret oversight as constraint.
This asymmetry creates misunderstanding.
The trainee feels constrained.
The attending feels stretched.
Both are true.
Delegation as a judgment skill
Expert attendings do not just delegate tasks.
They delegate problem spaces.
They decide which parts of thinking someone owns.
For example:
A trainee may gather data independently
while the attending retains diagnostic commitment.
A trainee may propose a plan
while the attending controls final communication.
A trainee may speak to the team
while the attending watches for framing drift.
Each domain carries different risk.
Each requires different trust.
Delegation is not distributing work.
It is distributing uncertainty.
What expert delegation looks like
At its best, delegation is explicit.
It sounds like:
You take first pass on framing.
I will review before we commit.
Here’s what I’m most worried about.
Here’s where I need to be looped in.
It makes boundaries visible.
It protects the patient.
It grows the trainee.
It protects the attending from silent overload.
Why some attendings never let go
Even attendings who understand this complexity
may find themselves unable to practice it.
Some stop delegating.
They do everything themselves.
They become efficient.
They become indispensable.
They become exhausted.
They also deprive trainees of cognitive practice.
Not because they don’t care.
Because the emotional cost of delegation has become too high.
The system rewards throughput.
It does not reward teaching risk.
The hidden emotional labor
Letting go feels like negligence.
Delegation requires tolerating discomfort:
not knowing exactly what is being said
not hearing every conversation
not controlling every decision
This is hard for people trained to be responsible.
In reality, letting go is how future consultants are built.
What this teaches about consult medicine
Delegation is not the opposite of responsibility.
It is responsibility extended through others.
It requires trust.
It requires monitoring.
It requires tolerance of imperfection.
It is one of the highest judgment skills in consult practice.
Because it is how expertise reproduces itself.
When attendings cannot delegate,
the system becomes safe in the short term
and brittle in the long term.
Consult medicine depends on people
who have been allowed to think before they were perfect.
That only happens if someone senior
is willing to carry the risk of letting go.
Not completely.
But enough.