How temperature became a way to speak about harm, distance, and loss of vitality
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
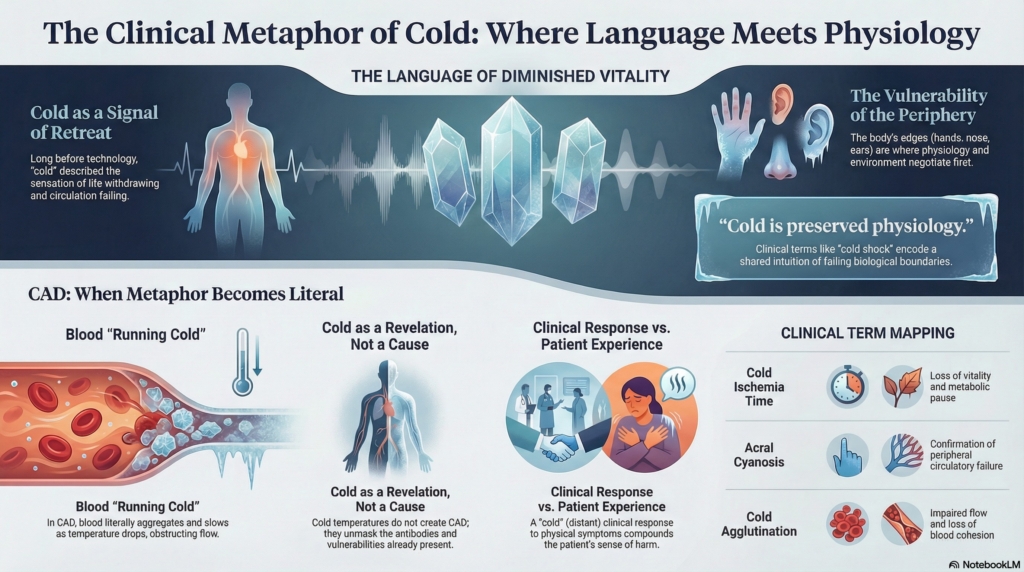
Cold has always carried meaning in medicine that exceeds temperature.
Long before thermometers or molecular explanations, clinicians and patients used cold to describe what it felt like when life withdrew, when circulation failed to reach the margins, when vitality thinned. Cold was not simply a physical state. It was a language for diminished flow, weakened presence, and impending danger.
Medical language about cold is not decorative. It is preserved physiology in words.
Cold as a metaphor for loss of life and motion
Across medical history, warmth signaled life. Cold signaled its retreat.
To be warm was to be animated, responsive, alive. To be cold was to slow, stiffen, and lose coherence. This association predates any knowledge of oxygen delivery or blood rheology. It arose from direct observation: cold limbs grew pale or blue, sensation dulled, movement faltered.
Even today, clinicians speak this language instinctively:
- “Cool extremities”
- “Cold shock”
- “Cold ischemia time”
- “Cold injury”
Each phrase encodes a shared intuition: cold marks the boundary where physiology begins to fail.
Blood “running cold”
Few metaphors are more enduring than blood running cold.
In everyday language, it signals fear, dread, or loss of courage. In medical language, it quietly signals something else: impaired circulation, slowed flow, withdrawal from the periphery. The metaphor is powerful precisely because it is grounded in bodily experience. When blood “runs cold,” sensation fades and color changes. The body feels less inhabited.
Cold agglutinin disease gives this metaphor literal form.1
Blood does not merely feel cold. It behaves differently. It aggregates, slows, and obstructs flow, especially where temperature drops first.
Cold, distance, and moral tone
Cold in medicine also carries moral weight.
To be “cold” as a clinician is to be distant, unfeeling, detached. To offer “cold comfort” is to provide reassurance without warmth or relief. These expressions reveal a deeper expectation: care should be warming. It should restore proximity, flow, and responsiveness.
This matters in CAD.
Patients often describe not just physical cold, but emotional coldness in encounters where symptoms are minimized because numbers look reassuring. The metaphors converge. Cold circulatory symptoms meet cold clinical responses. The result is a compounded harm that is felt, even if never named.
The periphery as a linguistic and physiologic edge
Language has always marked the body’s edges as vulnerable.
Hands grow cold first. Feet lose color. Ears ache. Noses numb. These sites recur in medical description and metaphor because they are where circulation thins and protection fails. The periphery is where the body negotiates with environment.
In CAD, pathology declares itself precisely there.
Acral cyanosis is not just a clinical finding. It is a confirmation of what language has long suggested about where cold does its damage first.
Cold as revelation, not cause
Metaphor also shapes how we understand causality.
Cold is often spoken of as something that causes illness. Historically, it was more often understood as something that reveals weakness. Cold exposed what warmth concealed. It made visible the limits of circulation, resilience, and balance.
This older framing aligns closely with CAD.
Cold does not create the disease. It reveals it. The antibodies and complement are already present. Temperature unmasks their consequences.
Whether clinicians say “cold triggers symptoms” or “cold reveals vulnerability” changes how patients understand their own bodies.
A patient told that cold “causes” the disease may experience winter as arbitrary danger. A patient told that cold reveals an underlying vulnerability may better understand warmth as mitigation rather than cure.
Language does not just describe physiology.
It interprets it.
Restoring meaning to words we still use
We still speak of:
- “warm versus cold ischemia”
- “cold intolerance”
- “cold-induced injury”
- “warming as therapy”
These are not poetic leftovers.
They encode real physiologic truths.
Metaphor is not decoration.
It is memory.
Cold means:
- impaired flow
- loss of cohesion
- retreat of vitality
- vulnerability at the margins
When blood is cold, it behaves badly. Language knew this before laboratories did.
Cold agglutinin disease does not just challenge physiology.
It challenges us to listen more carefully to the language medicine has been using all along.
Key reflections
- medical language about cold preserves physiologic insight
- metaphors of cold map onto circulatory vulnerability
- CAD literalizes expressions clinicians still use reflexively
- metaphor is not decoration; it is memory
linical Listening Note
When patients use phrases such as “my hands feel dead,” “my blood runs cold,” or “I feel frozen from the inside,” do not translate too quickly into symptoms and signs. First ask what the phrase is carrying: pain, color change, numbness, fatigue, fear, loss of function, or loss of trust. In CAD, metaphor may already be pointing toward physiology.
Reflect and Apply
A patient says:
“My hands feel dead in the cold.”
Before translating that phrase into clinical terminology, pause.
What might the patient already be describing?
impaired flow
loss of sensation
color change
functional withdrawal
fear that the body is becoming less alive at the margins
In CAD, patient metaphor may not obscure physiology. It may reveal it.
That feels more aligned with the essay than a quiz.
Additional Reading
- Gabbard AP and Booth GS. Cold Agglutinin Disease. Clin Hematol Int. 2020.
- NORD. Cold Agglutinin Disease – Symptoms, Causes, Treatment.
- Mosdosi B et al. Severe acrocyanosis precipitated by cold agglutinin secondary to infection with Mycoplasma pneumoniae in a pediatric patient. Croat Med J. 2017.