Overview:
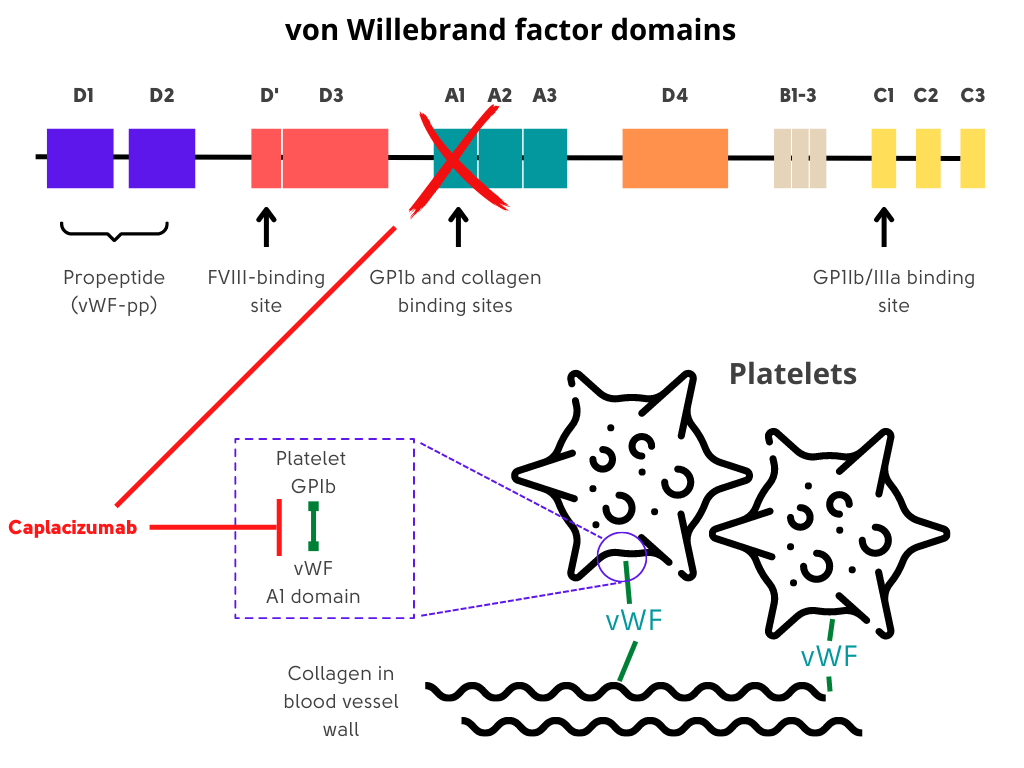
- Caplacizumab-yhdp (Cablivi) is a humanized, bivalent, variable-domain-only immunoglobulin fragment (nanobody, Ablynx) directed to the A1 region of von Willebrand factor (VWF), which specifically targets the A1 domain of VWF, preventing interaction with the platelet glycoprotein Ib-IX-V receptor (platelet-von Willebrand factor interactions) and the ensuing microvascular thrombosis in small arterioles and capillaries.
- Caplacizumab-yhdp (Cablivi) was FDA approved in 2019 for treatment of adults with immune TTP (iTTP) in combination with plasma exchange and immunosuppressive therapy.
- Represents the first drug to receive a regulatory approval for the treatment of iTTP.
- The half-life of caplacizumab is approximately 24 h; partially renally eliminated.1
Suggested dosing:
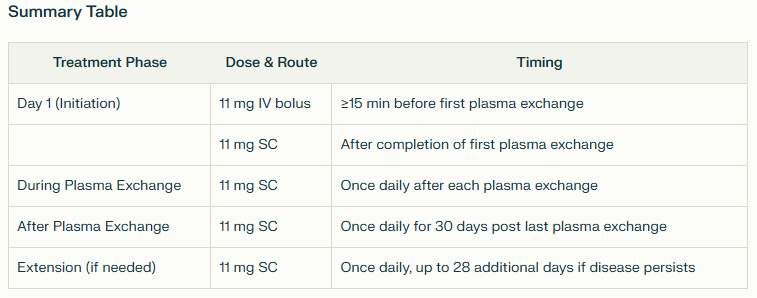
- Day 1 (initiation of therapy):
- 11 mg intravenous (IV) bolus at least 15 minutes prior to the first plasma exchange.2
- Followed by 11 mg subcutaneous (SC) injection after completion of the first plasma exchange on Day 1.
- During plasma exchange period:
- 11 mg SC injection once daily after each subsequent plasma exchange session.
- After completion of plasma exchange:
- 1 mg SC injection once daily for 30 days following the last plasma exchange.
- If there are signs of persistent underlying disease (such as suppressed ADAMTS13 activity), treatment may be extended for up to an additional 28 days.
- Patients or caregivers may administer SC injections after proper training.
Notes:
- Caplacizumab does not correct underlying ADAMTS13 deficiency nor does it eliminate anti-ADAMTS13 autoantibodies.
- Discontinuation of treatment after normalization of platelet count but with persistently low ADAMTS13 activity (<10% of normal) may result in exacerbation of disease.
- Immunosuppressive treatments such as rituximab and corticosteroids are still needed to manage underlying disease process.
- With the use of caplacizumab, low-dose aspirin (75 mg) is avoided until therapy has been completed.3
- International, multicenter, phase 2, randomized, placebo-controlled study of caplacizumab.
- Seventy-five patients with acquired [immune] TTP were enrolled.
- Patients were randomly assigned to subcutaneous caplacizumab (10 mg daily) or placebo during plasma exchange and for 30 days afterward
- Patients in both groups received the current standard of care of plasma exchange and immunosuppressive therapy.
- As compared with placebo, caplacizumab:
- Showed a short-term efficacy by reducing both:
- Time to platelet count normalization (primary end point); median time to response:
- 3.0 days in the caplacizumab group (95% confidence interval [CI], 2.7 to 3.9)
- 4.9 days in the placebo group (95% CI, 3.2 to 6.6)
- P value 0.005
- Early exacerbation rate
- Time to platelet count normalization (primary end point); median time to response:
- Did not have an effect on the risk of relapse of TTP (7 of 8 patients in Caplacizumab arm that relapsed within first month of stopping the medication had ADAMTS13 activity that remained below 10%)
- Associated with an increased tendency toward bleeding as compared with placebo, a potential outcome of blocking the interaction of von Willebrand factor with platelets.
- Showed a short-term efficacy by reducing both:
- Conclusions: “Caplacizumab induced a faster resolution of the acute TTP episode than did placebo. The platelet-protective effect of caplacizumab was maintained during the treatment period. Caplacizumab was associated with an increased tendency toward bleeding, as compared with placebo.”
- Phase 3 double-blind, randomized, parallel group, multicenter placebo-controlled trial designed to confirm the potential role of caplacizumab in the treatment of immune TTP (iTTP).
- 145 patients with iTTP randomized to receive caplacizumab (10 mg intravenous loading bolus, followed by 10 mg daily subcutaneously) or placebo during plasma exchange and for 30 days thereafter.
- As compared with placebo, caplacizumab was associated with:
- Greater percentage of patients to achieve normalization of the platelet count.
- Shorter median time to normalization of the platelet count:
- Caplacizumab: 2.69 days [95% confidence interval {CI}, 1.89 to 2.83
- Placebo: 2.88 days [95% CI, 2.68 to 3.56], P = 0.01)
- Lower recurrence of TTP during the trial
- Less plasma exchange
- Shorter hospitalization than those who received placebo
- Lower incidence of a composite of:
- TTP-related death
- Recurrence of TTP
- Thromboembolic event
- Higher rate of mucocutaneous bleeding (reported in 65% of the patients in the caplacizumab group and in 48% in the placebo group).
Guideline recommendations:
- For patients with immune TTP experiencing an acute event (first event or relapse), the panel suggests using caplacizumab over not using caplacizumab. (A conditional recommendation in the context of moderate certainty evidence.)
- Benefit of caplacizumab is accrued if it is started in the early phase of an acute TTP event (i.e., at the time when a diagnosis is confirmed). Practically, when treating physicians are considering caplacizumab, they should consider administration of the drug even before the results of plasma ADAMTS13 activity become available.
- Caplacizumab should only be given under the guidance of an experienced clinician.
- Clinicians using caplacizumab and patients who receive it must understand its unique mechanism of action as caplacizumab does not correct the underlying ADAMTS13 deficiency nor does it eliminate autoantibodies against ADAMTS13, the primary cause of iTTP.
- Discontinuation of caplacizumab treatment after platelet count normalization but with persistently low ADAMTS13 activity (<10 U/dL) may result in disease exacerbation. Therefore, the immunosuppressive therapies such as rituximab and corticosteroids are still required to control the underlying disease process.
- “The panel also noted that patients on caplacizumab experienced clinically important bleeding side effects”.
- “Caplacizumab is associated with side effects, significant cost, and requiring cotreatments to remove the underlying autoantibody”.
British Committee for Standards in Haematology:
- Caplacizumab reduces the duration of thrombocytopenia, exacerbations, refractory disease, admission duration, PEX procedures and volume of plasma used.
- Caplacizumab prevents a fall in platelet count associated with ADAMTS13 deficiency but does not modify the underlying immune disease process.
- Persistence of severe ADAMTS13 deficiency is associated with clinical relapse; therefore, caplacizumab may be continued beyond 30 days following cessation of PEX if ADAMTS 13 activity levels remain <10 iu/dL.
- Caplacizumab is being used in acute TTP without the need for PEX.
- Caplacizumab should be initiated on confirmation of acute iTTP and for up to 30 days following completion of PEX. In patients who remain severely ADAMTS13 deficient (<20 IU/dL) caplacizumab therapy may be continued. (Grade 1A)
Want to explore this further?
Check out the related sections in our TTP module:
- Journal Club on Scully et al. Caplacizumab treatment for acquired thrombotic thrombocytopenic purpura. N Engl J Med. 2019; 380: 335-346.
- Journal Club on Kühne et al. Management of immune thrombotic thrombocytopenic purpura without therapeutic plasma exchange. Blood. 2024(14):1486-1495.
- Treatment of TTP – Overview
- Video Lecture on TTP Treatment
- Section on Refractory TTP