Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Why this spoke matters
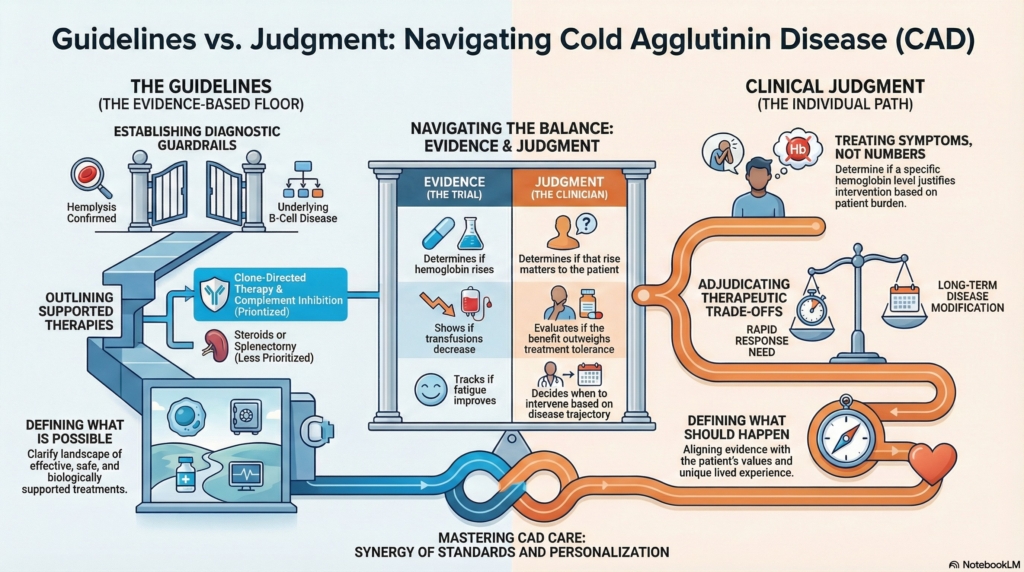
Cold agglutinin disease sits at a revealing intersection of strong biology and incomplete certainty.
Mechanisms are well described.
Therapies exist.
Consensus guidance outlines diagnostic and treatment pathways.
Yet real clinical decisions still depend on judgment.
Understanding why is essential for trainees. Early in training, guidelines feel like answers. With experience, they become frameworks. CAD is a disease in which overreliance on guidance can be as misleading as ignoring it.
Guidelines define possibility.
Judgment defines action.
What guidelines provide
Clinical guidelines clarify the landscape of what is known, what is effective, and what is no longer defensible.
In cold agglutinin disease, two documents anchor that landscape: the British Society for Haematology guideline for autoimmune hemolytic anemia and the First International Consensus recommendations for AIHA.
They provide shared structure by:
- defining diagnostic criteria
- standardizing terminology
- clarifying mechanisms of hemolysis
- outlining evidence-supported therapies
They also prevent outdated care. They identify which historical practices lack benefit and which treatments have biologic or clinical support.
For clinicians who encounter CAD infrequently, such documents provide essential guardrails.
Some guidance also reflects the therapeutic era in which it was written. Major CAD and AIHA guideline documents were developed before proximal complement inhibition became widely available in clinical practice. The BSH guideline predates sutimlimab entirely, and the First International Consensus recommendations were published before FDA approval of sutimlimab for CAD in 2022. This does not make the guidance obsolete, but it reminds clinicians that guidelines are time-stamped interpretations of available evidence, not permanent substitutes for judgment.
But guardrails are not destinations.
They define safe boundaries.
They do not determine the path within them.
Guideline Snapshot: What CAD guidelines actually recommend
Diagnosis
- confirm hemolysis with objective laboratory evidence
- perform monospecific DAT testing (anti-IgG and anti-C3d at minimum)
- distinguish primary CAD from secondary cold agglutinin syndromes
- evaluate for an underlying clonal B-cell disorder
- exclude secondary causes (autoimmune disease, malignancy, infection, drugs).
When to treat
- treat based on symptomatic anemia, transfusion need, or severe circulatory symptoms, not a fixed hemoglobin threshold
- observe mild, compensated CAD with monitoring and cold avoidance
Treatment principles
- corticosteroids are generally ineffective in CAD
- splenectomy is not recommended
- rituximab-based, clone-directed therapy is standard disease-directed treatment
- complement inhibition is a targeted option in selected cases, with newer proximal inhibitors expanding the therapeutic landscape beyond the era of older guidelines
- use warming precautions and supportive transfusion strategies
- consider thromboprophylaxis during severe hemolytic exacerbations
- folic acid supplementation is recommended in chronic hemolysis
Monitoring
- reassess longitudinally rather than by single laboratory values
- monitor for thrombosis, infections, and treatment toxicity
- evaluate cold-induced symptoms in addition to hemoglobin
Sources: First International Consensus Meeting, British Society for Haematology (BSH)
What guidelines cannot decide
Guidelines cannot determine whether treatment is warranted in a particular patient.
They do not adjudicate thresholds of tolerability, trade-offs between speed and durability of response, or competing therapeutic goals.
They cannot answer questions such as:
- Is Hb 9.5 acceptable for this patient?
- Does fluctuating anemia justify intervention?
- Should rapid complement blockade outweigh long-term disease modification?
- Does patient preference justify deviation from standard sequencing?
These decisions depend on variables that resist standardization:
- tempo of disease
- trajectory over time
- patient priorities
- tolerance for uncertainty
Guidelines standardize knowledge.
They cannot standardize values.
Evidence versus judgment
The evidence base in CAD is stronger than it once was.
Prospective studies exist.
Targeted therapies exist.
Endpoints are defined.
But trials answer narrow questions under defined conditions.
They can determine:
- whether hemoglobin rises
- whether transfusions decrease
- whether fatigue scores improve
They cannot determine whether those outcomes matter enough for a specific patient at a specific moment.
They also cannot answer many of the comparative questions clinicians most need resolved: which strategy should come first, how long to wait before switching, or how to weigh durability against immediacy in a given phenotype.
CAD trials are small.
Endpoints are population abstractions.
Comparative sequencing data are limited.
Evidence tells us what happens under studied conditions.
Judgment decides what to do in the unstudied space between them.
Why expert disagreement persists
When experts disagree in CAD, it is rarely because one is wrong.
It is because multiple interpretations can be correct.
One clinician may prioritize rapid hemolysis control.
Another may prioritize long-term remission.
One may emphasize laboratory stability.
Another may emphasize lived experience.
Some may start with clone-directed therapy.
Others may favor complement inhibition first in severe symptomatic disease.
These differences reflect weighting, not ignorance.
Disagreement, in this setting, is not noise.
It is the audible signal of judgment.
What mastery looks like
Mastery in CAD is not memorizing guideline tables.
It is knowing how to use them.
Expert clinicians recognize:
- guidelines provide a floor, not a ceiling
- evidence informs decisions but does not replace them
- deviation from guidance requires reasoning, documentation, and clarity of intent
- uncertainty can be acknowledged without eroding trust
The paradox of expertise is this: the more one understands the structure of evidence, the more visible its edges become.
The highest form of expertise in CAD is not certainty.
It is disciplined judgment within bounded knowledge.
Explicit principle
Guidelines define the safe space of care.
Clinical judgment determines how medicine is practiced within it.
Key Points
- guidelines define boundaries — they establish what is supported and what should be avoided
- judgment determines action — decisions depend on context, trajectory, and patient priorities
- evidence answers structured questions — trials clarify effects but cannot set individual thresholds
- expert disagreement reflects weighting — differences often arise from priorities, not errors
- mastery is disciplined interpretation — clinicians must integrate biology, evidence, and lived experience
Reflect and Apply
A patient with CAD has hemoglobin 9.6 g/dL, rising LDH, mild acrocyanosis, and stable energy level.
Would you treat now or monitor?
Before deciding, identify:
- which signal reflects mechanism
- which reflects trajectory
- which reflects lived burden
Which one should drive your decision?