What your answer reveals about how you frame the problem
In the poll, you were asked which test you would order for a patient with anemia. The three options were:
- SPEP (serum protein electrophoresis)
- Colonoscopy
- TSH
The responses varied widely. That variation is not random. Each test represents a different hypothesis about what kind of problem you think you’re facing.
Before interpreting the answers, it helps to anchor the discussion in expected yield.
What each test actually buys you (expected yield)
Approximate expected yield per 1000 similar patients.
| Test (what you’re buying) | What you’ll find (per 1000) | What matters clinically | Downstream cost / harm |
|---|---|---|---|
| SPEP/IFE (± sFLC) | ~74 will have a monoclonal protein (M-protein) detected if you screen broadly in anemia referrals1 | The majority are incidental MGUS-range findings, not the cause of anemia. Only ~1/1000 represents an underlying hematologic malignancy in that dataset. | High “label burden”: serial labs, annual follow-up, referrals, patient anxiety. (This is the MGUS:MM asymmetry problem in practice.) Population prevalence of MGUS is already a few percent in older adults, even before you add anemia.2 |
| Colonoscopy when ferritin is normal/high | If ferritin >100, advanced colonic neoplasia ~17/1000, which was similar to asymptomatic screening controls (~12/1000) in one large referral cohort3 | This suggests that, without iron deficiency, colonoscopy’s incremental diagnostic yield for “anemia as the clue” may be small, and often approximates age-appropriate screening yield. | Procedural risk, cost, false positives, and a tendency to treat “anemia” as its own cancer screen independent of iron deficiency signal. |
| TSH | In a large primary-care dataset, hypothyroidism was ~5.0% in anemic vs 4.2% non-anemic (absolute difference 0.8% = ~8 extra diagnoses/1000) | Even when you “find” hypothyroidism, it is often not the primary driver of anemia severity, and many patients would have been detected via routine care anyway (symptoms, prior testing). | Low incremental yield, lots of routine re-testing, and “incidental abnormality” management. |
Assumptions for this table: anemia present, no iron deficiency signal, no CKD, no other CRAB features, otherwise “well.” Change the population and the numbers move, but the relationships remain. Rounded teaching estimates based on prevalence data and referral cohorts; exact numbers vary by age and clinical context.
- SPEP is the classic high-incidental-finding test in this setting: you will “hit” MGUS frequently, but malignancy yield can be ~1 per 1000 in broad anemia screening, meaning most downstream work is follow-up of findings that are not causing the anemia.
- Colonoscopy is highest yield when the anemia carries an iron-deficiency signal. When ferritin is clearly normal/high, advanced neoplasia rates may look close to baseline screening, which reframes colonoscopy from “anemia workup” back to “age-appropriate CRC screening.”
- TSH is common, but its incremental value as an “anemia test” is small (the absolute difference in hypothyroidism prevalence in anemic vs non-anemic patients was under 1%).
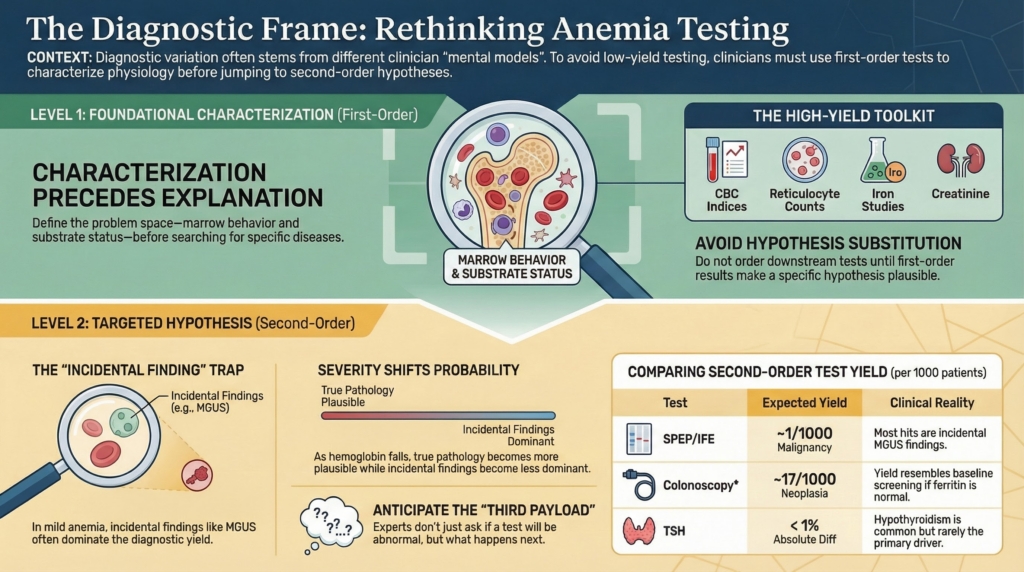
A critical modifier: severity changes yield
The table above assumes a stable patient with mild unexplained anemia. That assumption matters. The probability that any of these tests uncovers a causative diagnosis rises as anemia becomes more severe or physiologically consequential.
Severity shifts diagnostic probability.
As hemoglobin falls:
- marrow disorders become more plausible
- occult malignancy becomes more plausible
- systemic disease becomes more plausible
- incidental findings become less dominant relative to true pathology
| Severity | Diagnostic implication |
|---|---|
| Mild anemia | incidental findings dominate yield |
| Moderate anemia | mixed signal |
| Severe anemia | true pathology dominates yield |
Experienced clinicians change testing strategy based not only on what abnormality exists, but on how abnormal it is.
Severity is not just a number.
It is a probability signal.
What each choice actually assumes
SPEP
Ordering SPEP means you think a plasma cell disorder plausibly explains the anemia. The statistical reality is that monoclonal proteins are far more common than malignant plasma cell disease.
What typically happens:
- most positives are MGUS
- most MGUS is incidental
- most incidental findings trigger surveillance
Broad SPEP testing therefore functions less as cancer detection and more as monoclonal protein detection followed by monitoring.
Colonoscopy
Ordering colonoscopy assumes gastrointestinal pathology is a plausible cause of anemia. That assumption is strongest when there is evidence of iron deficiency.
Without iron deficiency:
- detection rates resemble screening populations
- many findings are unrelated to anemia
- procedural risk remains unchanged
In other words, colonoscopy without iron deficiency often behaves more like routine cancer screening than targeted anemia evaluation. If yield approximates baseline screening rates, the anemia is not adding diagnostic information. It is only providing justification.
TSH
Ordering TSH assumes endocrine suppression of erythropoiesis is a leading explanation. Thyroid disease is common, so abnormal TSH values are common. But hypothyroidism severe enough to explain anemia is much less common.
Typical pattern:
- abnormal results are frequent
- causative results are uncommon
- many abnormalities are mild or incidental
So the test often detects thyroid disease that exists but does not explain the hematologic problem.
What the poll actually revealed
Different clinicians chose different tests because they were solving different problems in their minds:
- some were screening for malignancy
- some were searching for bleeding
- some were scanning for systemic disease
The divergence reflects variation in problem framing, not disagreement about medicine.
Each answer corresponds to a recognizable cognitive posture:
- SPEP mindset: rule out the dangerous diagnosis
- Colonoscopy mindset: find the hidden source
- TSH mindset: check common systemic causes
The poll was not testing knowledge.
It was revealing mental models (how clinicians frame problems).
The missing step most algorithms skip
Characterization precedes explanation.
All three tests share something important: they are second-step tests.
They make sense only after the anemia has been characterized.
Before any of them, the highest-yield first move is physiologic framing:4
First-order characterization tests
- CBC indices (MCV, RDW, MCHC)
→ morphology class and production clues - Reticulocyte count
→ production vs destruction vs loss - Peripheral smear review
→ structural biology, not numbers - Iron studies (ferritin, TSAT)
→ substrate availability vs sequestration - Creatinine
→ EPO axis integrity - CRP/ESR (context-dependent)
→ inflammatory physiology signal - B12/folate
→ substrate availability vs sequestration
What first-order tests actually do
These first-order tests do something fundamentally different.
They do not search for or name diseases.
They define the problem space, namely:
- marrow behavior
- substrate status
- systemic physiology
- tempo
- physiologic reserve
Without that step, ordering broad downstream tests is not hypothesis testing.
It is hypothesis substitution.
Second-order tests are hypothesis-testing tests
These are the ones from our poll:
- SPEP
- colonoscopy
- TSH
Each assumes a pre-existing frame:
| Test | Assumed frame |
|---|---|
| SPEP | plasma cell disorder plausible |
| Colonoscopy | bleeding/malignancy plausible |
| TSH | endocrine suppression plausible |
They are rational only after first-order tests define a terrain that makes one of those hypotheses plausible.
The deeper diagnostic principle
No test is neutral. Every test carries three payloads:
- probability of detecting true disease
- probability of detecting incidental disease
- probability of triggering downstream consequences
Novices focus on the first.
Experts anticipate the third.
So experienced clinicians don’t ask only:
Could this be abnormal?
They ask:
If it is, what happens next?
Bottom line
In a stable patient with anemia and no defining clues:
- SPEP most often finds MGUS, not myeloma
- colonoscopy is highest yield when iron deficiency is present
- TSH abnormalities are common, causative anemia is not
So the best first test is usually not the one that can be positive.
It is the one most likely to change management for this patient, in this severity, in this clinical terrain.