I recently saw a 34 yo F with a history of radiologically and biopsy-proven primary sclerosing cholangitis who was found to have an elevated PT/INR and aPTT (no bleeding symptoms, no warfarin/antibiotics). Her vitamin A, D and E levels were all low.
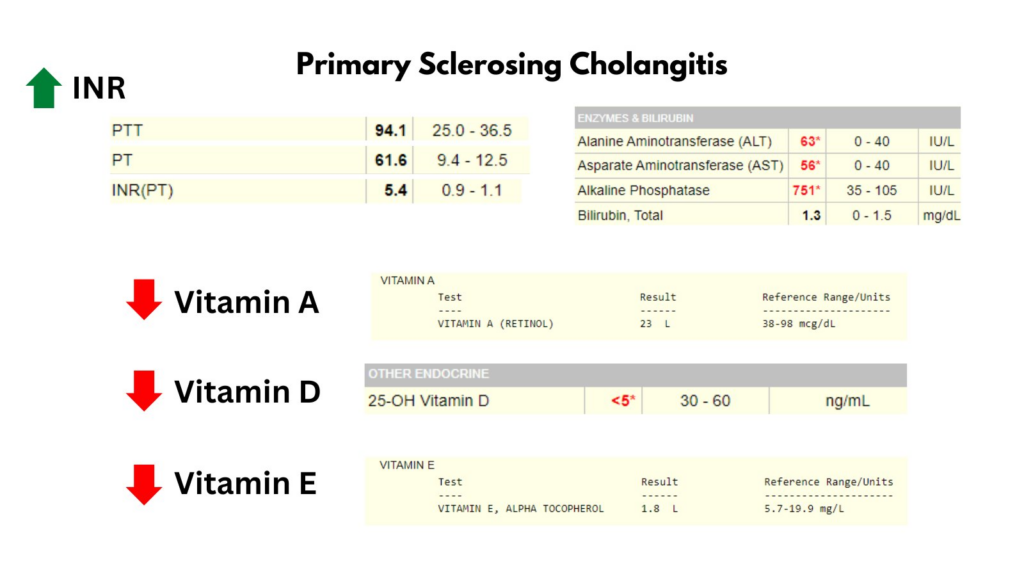
She was treated with vitamin K 5 mg IV x 2, and her INR normalized within 12 hours. Based on her low levels of vitamin A, D and E she was diagnosed with primary sclerosing cholangitis-associated fat-soluble vitamin deficiency.
Q: WHAT IS PRIMARY SCLEROSING CHOLANGITIS (PBC)?
A: Chronic progressive liver disease where inflammation and fibrosis lead to multifocal biliary strictures.

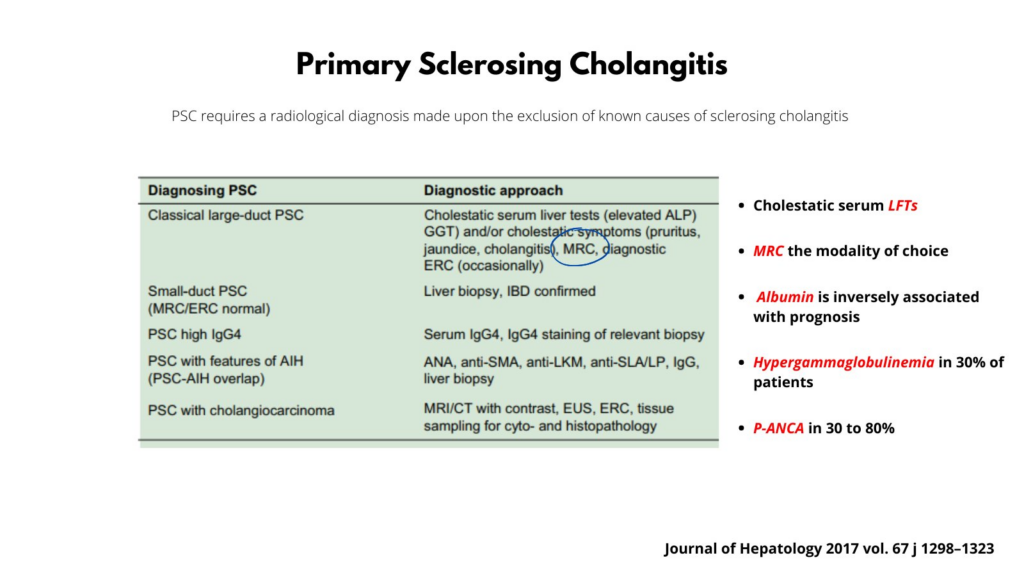
Q: HOW IS PBC DIAGNOSED?
A: With imaging and biopsy (as in this case). Labs usually show a cholestatic picture with elevated alkaline phosphatase.
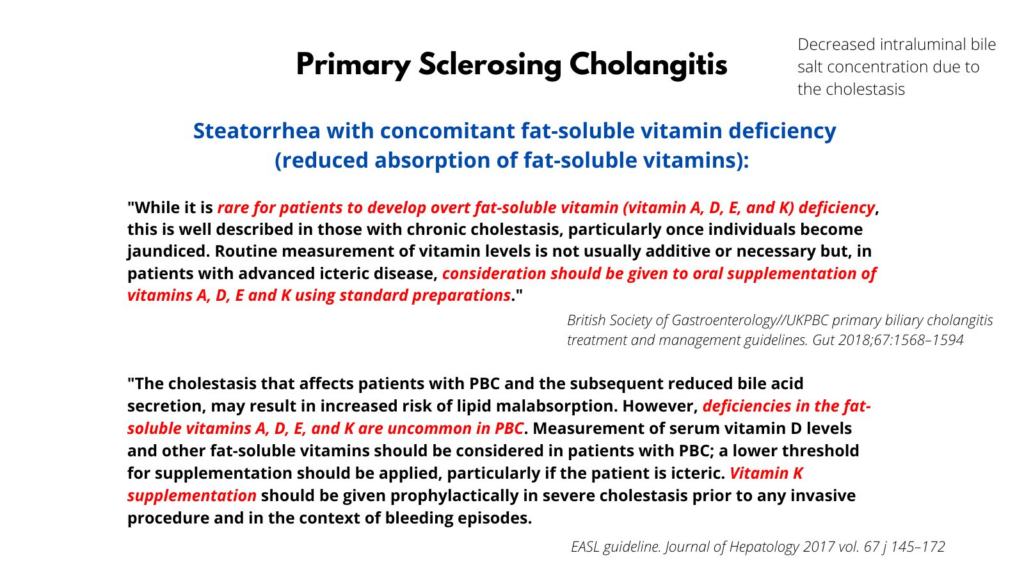
Q: WHAT DO THE GUIDELINES SAY ABOUT FAT SOLUBLE VITAMINS IN PBC?
A: Such deficiencies are rare, but be on the lookout for them, and consider oral supplementation depending on the clinical context.
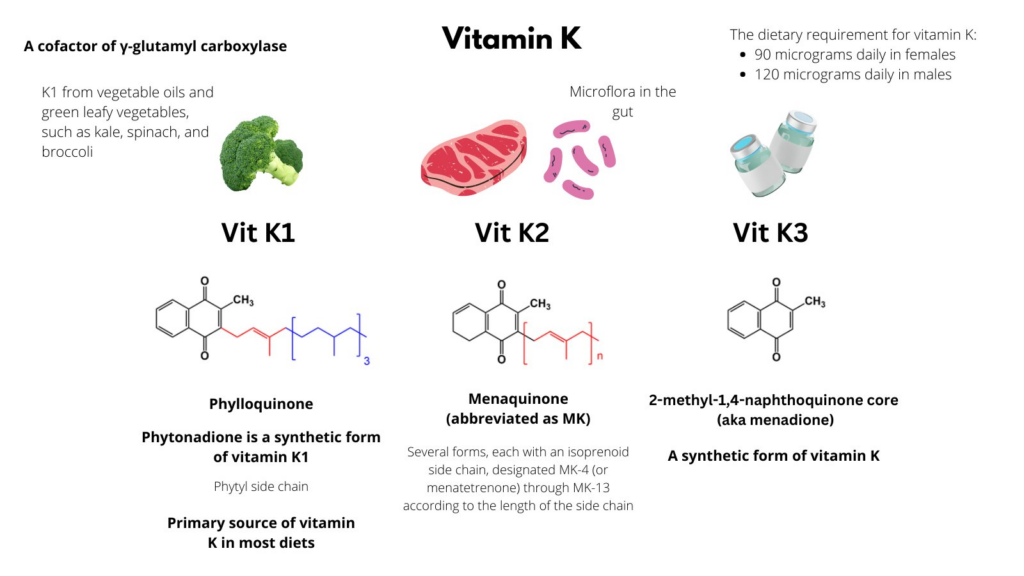
Q: HOW MANY FORMS OF VITAMIN K ARE THERE?
A: Three: two natural (K1, K2) and one synthetic (K3) form. K1 is from plants, K2 (which has varying lengths of the sidechain) is from animal products and glut flora. A synthetic form of K1 is typically used for treatment.
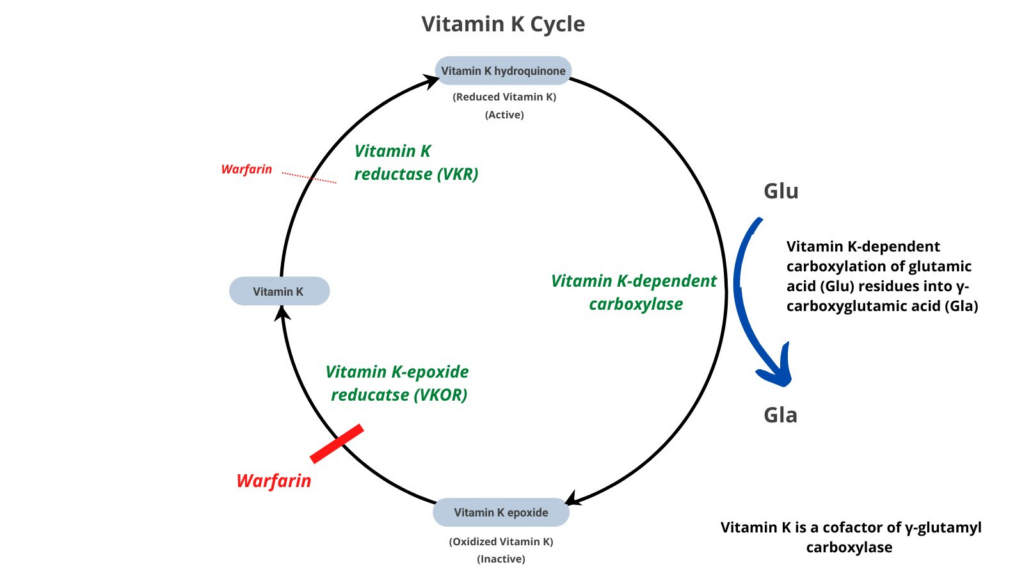
Q: REMIND ME HOW VITAMIN K WORKS?
A: It is a cofactor of γ-glutamyl carboxylase which results in carboxylation of glutamic acid (Glu) residues into γ-carboxyglutamic acid (Gla) in clotting factors II, VII, IX, and Xl; anticoagulants PC and PS; and certain bone proteins.
Q: THE PATIENT NOT ONLY HAD AN ELEVATED PT/INR, BUT ALSO AN ELEVATED aPTT. WHY?
A: Because vitamin K-dependent clotting factors function not only in the extrinsic pathway (VII) but also the intrinsic (IX) and common pathways (II, X).

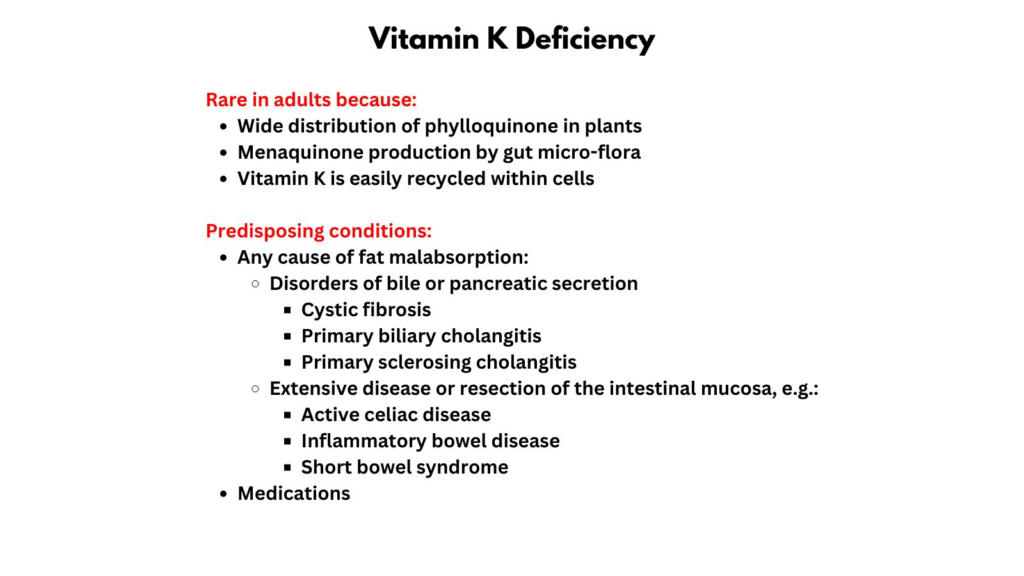
Q: WHAT ARE OTHER CAUSES OF VITAMIN K DEFICIENCY IN ADULTS?
A: Any cause of fat malabsorption, including disorders of bile or pancreatic secretion, extensive disease or resection of the intestinal mucosa, and medications (e.g., antibiotics).