For Your Healthcare Provider
Have your patient scan this QR code with their smartphone camera to instantly access this educational guide on their device.
A guide for patients with an elevated platelet count
Access the Resources
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
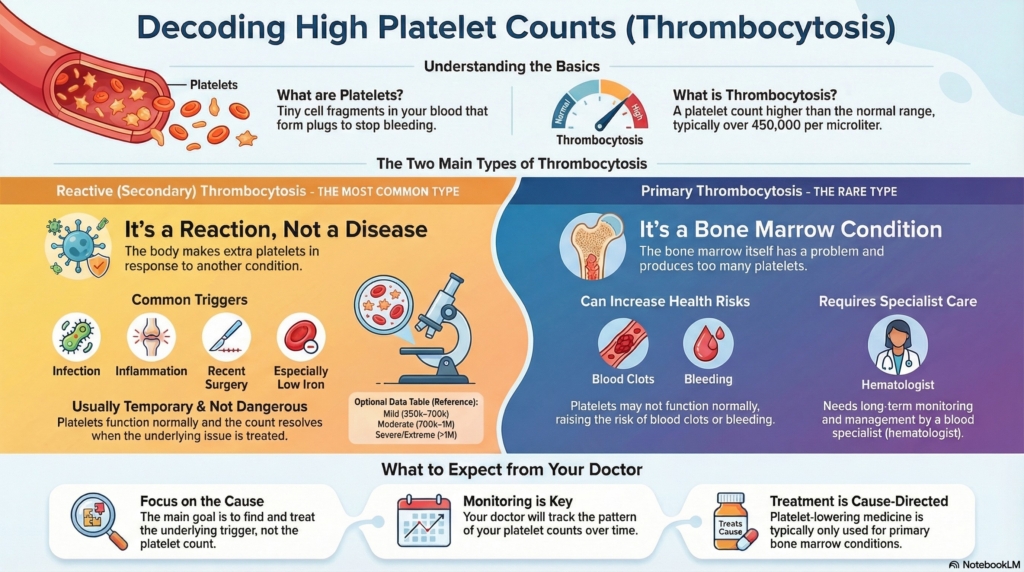
A high platelet count, called thrombocytosis, is common and often temporary.
Most people with thrombocytosis have a reactive (secondary) cause such as infection, inflammation, or low iron, and their count returns to normal with treatment of the underlying issue.
We will walk you through what platelets do, why the count may be high, and what to expect from evaluation, monitoring, and follow-up.
This guide applies to outpatient evaluation of high platelets. It does not apply to emergency or rapidly worsening symptoms.
First things first
A high platelet count is often discovered on a routine blood test. Many people with thrombocytosis have no symptoms, and the causes are usually non-dangerous and treatable. Your doctor’s first step is to understand why the count is elevated and whether it requires treatment, monitoring, or both.
What are platelets?
Platelets are tiny cell fragments in the blood that help stop bleeding. When a blood vessel is injured, platelets gather at the site, stick together, and begin forming a plug to prevent blood loss.
What is thrombocytosis?
Thrombocytosis means a platelet count higher than the usual range. It is usually defined as greater than 450,000 platelets per microliter (450 × 10⁹/L). Some labs use a threshold of 400 × 10⁹/L.
There are two main patterns of high platelets:
- reactive (secondary) thrombocytosis: the body makes extra platelets in response to another condition, such as infection, inflammation, or iron deficiency; platelets are working normally, and the count usually returns toward normal once the underlying problem is treated
- primary thrombocytosis: much less common, this occurs when the bone marrow itself has a problem and makes too many platelets on its own, as in essential thrombocythemia (ET) or another myeloproliferative neoplasm. These conditions need long-term monitoring by a hematologist
Most people with a high platelet count have reactive thrombocytosis, not a bone marrow cancer.
How platelets are measured
Platelets are counted as part of a complete blood count (CBC). The laboratory reports the value as “platelets × 10⁹/L” or simply “platelets.” Your result may be written as, for example, 500 × 10⁹/L or 500,000.
Ranges that matter
- mild thrombocytosis: 450,000–700,000
- moderate thrombocytosis: 700,000–1,000,000
- severe thrombocytosis: 1,000,000–1,500,000
- extreme thrombocytosis: above 1,500,000
These ranges help guide evaluation and monitoring, but the cause of the high count is more important than the number alone.
Why it happens (causes)
Reactive (secondary) causes
These are the most common reasons platelet counts rise and usually reflect the body responding to stress or inflammation:
- infection of any type
- inflammation from conditions such as arthritis, chronic illness, or cancer
- iron deficiency (a frequent and important cause)
- recent surgery or injury
- recent bleeding or recovery after a serious illness
- removal of the spleen (splenectomy)
- certain medications (such as epinephrine, some growth factors, and a few chemotherapy-related drugs)
- smoking
Clonal (bone marrow–related) causes
Much less commonly, thrombocytosis reflects a condition in which the bone marrow makes platelets on its own:
- essential thrombocythemia or another myeloproliferative neoplasm

On the right, essential thrombocythemia shows a clonal process, in which one abnormal megakaryocyte clone (large cells of the same color) produces excessive numbers of platelets.
Large shapes represent megakaryocytes. Small plus- or star-shaped symbols represent platelets circulating in the blood.
Does it cause symptoms?
Most people with mild or moderate thrombocytosis have no symptoms. When symptoms do occur, they are usually from the underlying condition (for example, fever and tiredness from infection or joint pain from inflammation), rather than from the platelet count itself.
In a small number of people, especially when platelet counts are extremely high (over 1,000,000–1,500,000), symptoms can include:
- headaches or visual changes
- tingling or burning in the hands or feet
- easy bruising, nosebleeds, or gum bleeding
These symptoms are much more common in primary bone marrow conditions—such as essential thrombocythemia—than in reactive thrombocytosis.
In reactive thrombocytosis, studies have not shown a clear increase in clotting risk from the platelet count alone, even at very high levels.
In primary bone marrow conditions, platelets may not function normally, which can increase the risk of both clotting and bleeding.
When thrombocytosis is caused by a bone marrow condition, additional symptoms may include:
- redness, heat, or burning pain in the hands or feet (erythromelalgia)
- swelling or pain in one leg, which could signal a blood clot in a vein
- sudden shortness of breath or chest pain
- sudden weakness on one side of the body, trouble speaking, or vision loss (possible arterial clot)
These problems are rare and occur mainly when platelets are abnormal in function—not just high in number. Any new or concerning symptoms should be discussed with your doctor right away.
Symptoms in children and adults
Symptoms vary widely and may include:
- fatigue or low energy
- pale skin
- yellowing of the eyes or skin
- darker urine
- abdominal discomfort or early satiety from an enlarged spleen
- episodes of worsening anemia during illness
- abdominal pain, especially after eating fatty foods (possible gallstones)
- nausea or vomiting (possible gallstones)
Some people have very mild symptoms, while others need more frequent monitoring or treatment.
Is it dangerous?
For most people with reactive thrombocytosis, a high platelet count is not dangerous and improves once the underlying cause is treated. The platelets are responding normally; there are simply more of them for a period of time.
In primary thrombocytosis (such as essential thrombocythemia), the platelets themselves may be abnormal, and the risk of blood clots is higher even at similar platelet levels. These conditions require close monitoring and sometimes treatment by a hematologist.
At very high platelet counts (around or above 1,000,000–1,500,000), platelets can also stop working normally and use up certain clotting proteins, which may increase the risk of bleeding. This paradox—that very high platelets can cause bleeding—is one reason doctors take extreme elevations seriously, especially if you have nosebleeds, easy bruising, or other bleeding symptoms.
How your doctor evaluates it
Evaluation usually includes:
- repeat CBC to confirm the platelet result and look at other blood counts
- review of recent illnesses, inflammation, surgery, or bleeding
- iron studies (such as ferritin) to check for iron deficiency
- review of medications and smoking history
- physical examination looking for signs of infection, inflammation, or an enlarged spleen
Over time, your doctor will also look at the pattern of your platelet counts:
- if the count falls as infection, inflammation, or iron deficiency improve, this supports a reactive cause
- if the count stays high for several months without a clear explanation, or if it is very high, your doctor may consider a primary bone marrow condition
In selected cases, especially with persistent marked elevation, your doctor may:
- order genetic tests (such as JAK2, CALR, or MPL)
- refer you to a hematologist
- rarely, recommend a bone marrow biopsy
Most people do not need these specialized tests; they are reserved for specific situations.
How is it treated
Treatment depends on the cause:
- treating infections
- managing chronic inflammation
- correcting iron deficiency with diet or supplements
- adjusting or stopping contributing medications, if appropriate
- supporting recovery after surgery or major illness
Most people with reactive thrombocytosis do not need platelet-lowering treatment. The count usually comes down on its own as the underlying condition improves.
Platelet-lowering medicines or aspirin are typically reserved for primary bone marrow conditions, very high counts with symptoms, or specific clotting-risk situations decided by a hematologist.
Daily life and self-care
Most people do not need major lifestyle changes because of thrombocytosis.
Helpful steps include:
- staying hydrated
- avoiding smoking
- following your doctor’s plan for treating any underlying condition
- maintaining regular, moderate exercise as tolerated
- moving around on long trips to reduce general clot risk
- keeping a list of symptoms and bringing it to appointments
- reporting new bruising, bleeding, or unusual headaches
No special diet or activity restriction is required solely because of thrombocytosis.
When should I contact my doctor?
You should call your doctor if you have:
- unexplained bruising or bleeding
- frequent nosebleeds or bleeding gums
- new or severe headaches
- vision changes such as blurring or brief loss of vision
- chest pain or shortness of breath
- swelling or pain in one leg
- platelet counts rising above 1,000,000–1,500,000 on repeat testing
Seek emergency care for sudden weakness on one side, trouble speaking, severe shortness of breath, crushing chest pain, or heavy uncontrolled bleeding.
What is the usual plan going forward?
Most people with reactive thrombocytosis need monitoring and cause-directed treatment, rather than treatment of the platelets themselves.
A typical plan might include:
- rechecking your blood count in about 4–8 weeks after treating the suspected cause (such as infection or iron deficiency)
- if the platelet count is improving, extending rechecks to every 2–3 months until it returns to a normal or stable pattern
- if no clear cause is found and the count remains high for several months, your doctor may refer you to a hematologist for further evaluation
- if a primary bone marrow condition such as essential thrombocythemia is diagnosed, you will have regular hematology follow-up over the long term
Your doctor will tailor the schedule to your situation, other health conditions, and how your counts change over time.
Making sense of it
Think of platelets as emergency repair crews that rush out to fix leaks in blood vessels.
When there is an “alarm” in the body, such as infection, inflammation, or low iron, extra crews are called in and the number of workers goes up for a while.
Most of the time, once the alarm settles and the problem is fixed, the extra crews go home and the number of workers returns closer to normal.
Only rarely is the problem in the “control center” itself, where the bone marrow sends out too many workers all the time, which needs long-term specialist attention.
Thrombocytosis means your body is making more platelets than usual. In most people, this is a reactive response to something else going on, like infection, inflammation, or iron deficiency, and the count improves as that problem is treated. A much smaller group of people have a bone marrow condition that keeps platelets high and needs ongoing care from a hematologist. Your doctor’s job is to figure out which type you have, treat any underlying cause, and decide whether extra follow-up is needed.
Key takeaways
- most high platelet counts are reactive and improve when the underlying cause is found and treated
- thrombocytosis means platelets above 450,000, with higher ranges helping guide evaluation but not telling the whole story on their own
- iron deficiency is a common and important cause, and correcting it can lower the platelet count
- primary bone marrow causes such as et are much less common, and they need long-term follow-up with a hematologist
- very high counts can sometimes increase bleeding risk, not just clotting risk, because platelets may stop working normally
- regular monitoring helps your doctor see the pattern over time, decide whether more testing is needed, and keep you safe
For clinicians: Read our detailed guide on how to communicate about thrombocytosis to patients.