For Your Healthcare Provider
Have your patient scan this QR code with their smartphone camera to instantly access this educational guide on their device.
A guide for patients with polycythemia vera (PV)
Access the Resources
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Polycythemia vera (PV) is a myeloproliferative neoplasm, a chronic blood cancer in which the bone marrow makes too many blood cells, especially red blood cells.
This makes the blood thicker and more prone to clotting, which increases the risk of serious blood clots if PV is not treated.
Even though many people feel well at the time of diagnosis, PV is never “benign.”
It requires lifelong hematology care, regular blood tests, and treatments that keep blood thickness in a safer range and lower the risk of clotting.
This guide applies to outpatient evaluation and does not apply to emergency or rapidly worsening illness.
First things first
Polycythemia vera (PV) is a myeloproliferative neoplasm, a chronic blood cancer in which the bone marrow makes too many blood cells, especially red blood cells.
This makes the blood thicker and more prone to clotting, increasing the risk of serious blood clots if PV is not treated.
Even though many people feel well at the time of diagnosis, PV is never “benign.”
It requires lifelong care with a hematologist, regular blood tests, and treatments that keep blood thickness in a safer range and lower the risk of clotting.
What is polycythemia vera?
PV begins in the bone marrow, where a change in a gene called JAK2 causes blood-forming cells to grow even when the body does not need more. This leads to:
- too many red blood cells
- sometimes too many platelets
- sometimes too many white blood cells
PV is almost always driven by an acquired JAK2 mutation. It is not caused by anything you did, and it is not usually inherited.
People are often diagnosed after routine blood tests show high hemoglobin or hematocrit. A hematologist confirms the diagnosis with blood work, JAK2 testing, and sometimes a bone marrow biopsy.
Why it happens (causes)
Polycythemia vera (PV) is a chronic bone marrow disorder in which blood-forming cells grow when the body does not need more.
PV is almost always caused by a change in a gene called JAK2, which controls how blood cells grow and divide. This mutation:
- is acquired during life, not present at birth
- cannot be prevented
- is not usually passed on to children
- sends constant “grow” signals that make the marrow overproduce cells
The overproduction primarily affects red blood cells, but platelets and white blood cells may also be increased.
Does it cause symptoms?
Some people have no symptoms at first, while others notice patterns that are common in PV, including:
- headaches, dizziness, or trouble concentrating
- itching after warm showers or baths (aquagenic pruritus)
- burning pain, redness, or warmth in the hands or feet (erythromelalgia)
- redness or flushing of the face or extremities
- fatigue or low energy
- night sweats or unintentional weight loss
- fullness or discomfort under the left ribs, from an enlarged spleen
- joint pain or gout, related to high uric acid levels
Symptoms often improve when treatment brings the blood thickness into a safer range.
Is it dangerous?
The main danger in PV is blood clots.
These can occur in arteries or veins and may cause:
- stroke-like symptoms (weakness, trouble speaking, sudden vision changes)
- heart attack–type symptoms (chest pain, shortness of breath)
- clots in the legs (DVT)
- clots in the lungs (PE)
- less common clots in veins of the liver or abdomen
Doctors classify PV by clot risk:
- low-risk: younger than 60 and no history of blood clots
- high-risk: age 60 or older, or a prior blood clot
Over time, PV can also lead to changes in the bone marrow, such as myelofibrosis or, rarely, acute leukemia.
These complications are uncommon with modern treatment but reinforce the importance of lifelong follow-up.
How your doctor evaluates it
Evaluation usually includes:
- a detailed medical history and exam, including spleen size
- blood tests for hemoglobin, hematocrit, platelets, white blood cells, and erythropoietin (EPO)
- testing for the JAK2 mutation
- imaging if spleen enlargement is suspected
- sometimes a bone marrow biopsy
Your doctor also reviews cardiovascular risk factors (blood pressure, cholesterol, diabetes, smoking), since these strongly influence clot risk.
How is it treated
Treatment focuses on preventing clots, lowering blood thickness, and controlling symptoms.
Phlebotomy (blood removal)
Phlebotomy is the foundation of treatment.
Removing blood lowers the hematocrit, which is closely linked to clot risk.
- early on, phlebotomy may be frequent until the hematocrit is controlled
- long-term, it is done periodically to keep the hematocrit below 45%
- iron stores usually fall, which helps slow red blood cell production
Do not take iron supplements unless your hematologist specifically directs you to.
Low-dose aspirin
Most people with PV take low-dose aspirin to reduce clot risk and improve certain circulation-related symptoms.
Medicines that slow blood cell production
Used in higher-risk patients or those needing frequent phlebotomy, including:
- hydroxyurea, an oral medication
- interferon, often preferred in younger adults or pregnancy planning
- other treatments, such as JAK inhibitors, in selected situations
Your treatment plan is individualized and may change over time.
Daily life and self-care
Most people with PV can work, exercise, travel, and enjoy daily life.
Key steps include:
- cardiovascular health: do not smoke, and manage blood pressure, cholesterol, and diabetes
- hydration and movement: stay well hydrated and avoid long periods without moving
- medication and follow-up adherence: take medicines as prescribed and keep all lab and clinic visits
Pregnancy requires specialized care.
PV in pregnancy is higher risk and should be managed by a hematologist and a high-risk obstetrician.
Some PV medicines are not safe in pregnancy and need advance planning.
When should I contact my doctor?
Contact your hematology team promptly if you have:
- new or worsening headaches, dizziness, or vision changes
- new chest discomfort or shortness of breath
- new leg pain, redness, or swelling
- increasing fullness or discomfort under the left ribs
- unusual or heavy bleeding
- fevers, night sweats, or unexplained weight loss
- a clear change in your usual PV symptoms
Call 911 or go to the emergency department immediately if you have:
- stroke-like symptoms (face drooping, arm weakness, trouble speaking)
- sudden chest pain or difficulty breathing
- coughing up blood
- sudden severe leg or abdominal pain
- bleeding that will not stop with pressure
Tell emergency staff that you have polycythemia vera and list your medications.
What is the usual plan going forward?
PV is a lifelong condition.
After the initial treatment phase:
- blood counts are checked regularly
- phlebotomy and medications are adjusted as needed
- your doctor monitors for disease evolution
- cardiovascular risk factors are addressed at every visit
The goal is to prevent clots, control symptoms, and detect changes early.
With good care, many people with PV remain stable for decades.
Making sense of it
Think of your bloodstream as a busy highway.
In PV, there are too many cars, packed too closely together, which raises the chance of accidents.
Treatment removes some cars and slows how quickly new ones appear, helping traffic flow more smoothly and safely.
PV means your marrow is making more blood cells than your body needs.
Treatments like phlebotomy, aspirin, and cell-slowing medicines reduce clot risk and help you live a full, active life.
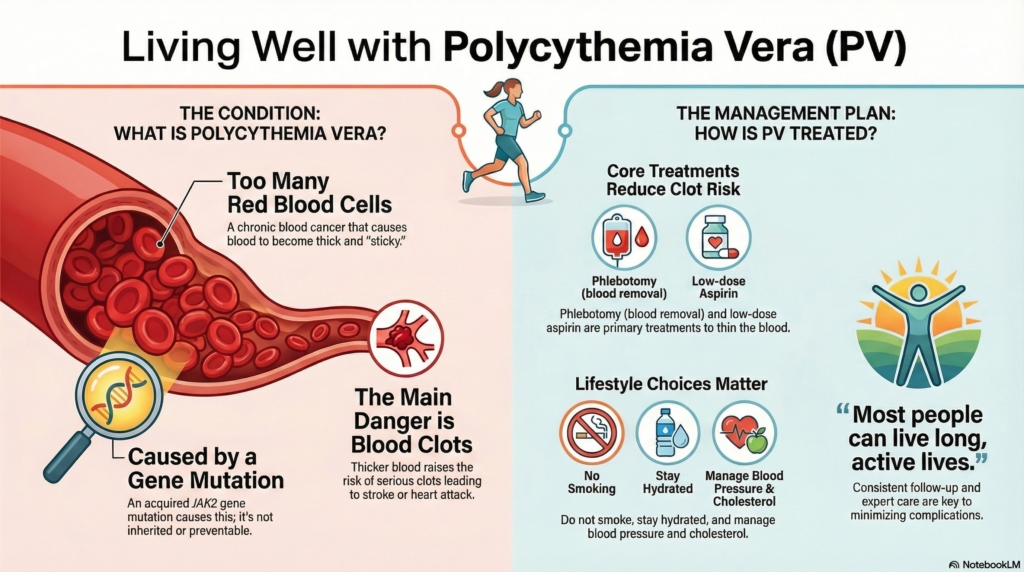
Key takeaways
- chronic blood cancer: PV causes overproduction of blood cells and thicker blood
- JAK2-driven: the mutation is acquired during life and not your fault
- clot prevention is central: treatment focuses on phlebotomy, aspirin, and sometimes medication
- risk-based treatment: age and prior clots guide how aggressive therapy needs to be
- lifestyle matters: not smoking, staying hydrated, and managing heart risk factors are important
- pregnancy needs planning: specialized care is essential
- long-term outlook is good: with consistent follow-up, many people live long, active lives
For clinicians: Read our detailed guide on how to communicate about polycythemia vera to patients.