For Your Healthcare Provider
Have your patient scan this QR code with their smartphone camera to instantly access this educational guide on their device.
A guide for patients with hereditary hemochromatosis
Access the Resources
Note: The video and audio linked above were generated with the assistance of AI. Clinical accuracy has been reviewed, but no AI-generated content can be guaranteed to be fully error-free.
Many people now see their ferritin and transferrin saturation results online, and even small elevations may appear in red.
Ferritin can be mildly elevated for many reasons unrelated to iron overload, including inflammation, infection, fatty liver, or recent illness. Hereditary hemochromatosis is common, highly treatable, and often silent for many years, and most people diagnosed early stay healthy with simple monitoring and phlebotomy when needed.
This guide applies to outpatient evaluation and does not apply to emergency or rapidly worsening illness.
First things first
Hereditary hemochromatosis usually progresses very slowly. Most people who are diagnosed early never develop organ damage and remain healthy for decades with simple monitoring and treatment when needed.
Seeing an elevated ferritin on a patient portal can be alarming, especially when the number appears in red. Mild to moderate elevations, often in the range of a few hundred, are common and do not by themselves mean that iron overload is causing harm. Ferritin can rise for many reasons unrelated to hereditary hemochromatosis, including inflammation, infection, fatty liver disease, or recent illness.
Hereditary hemochromatosis is typically confirmed when both ferritin and transferrin saturation are persistently elevated together, rather than based on a single result. Your doctor will usually repeat testing and, when appropriate, order genetic testing to clarify the diagnosis.
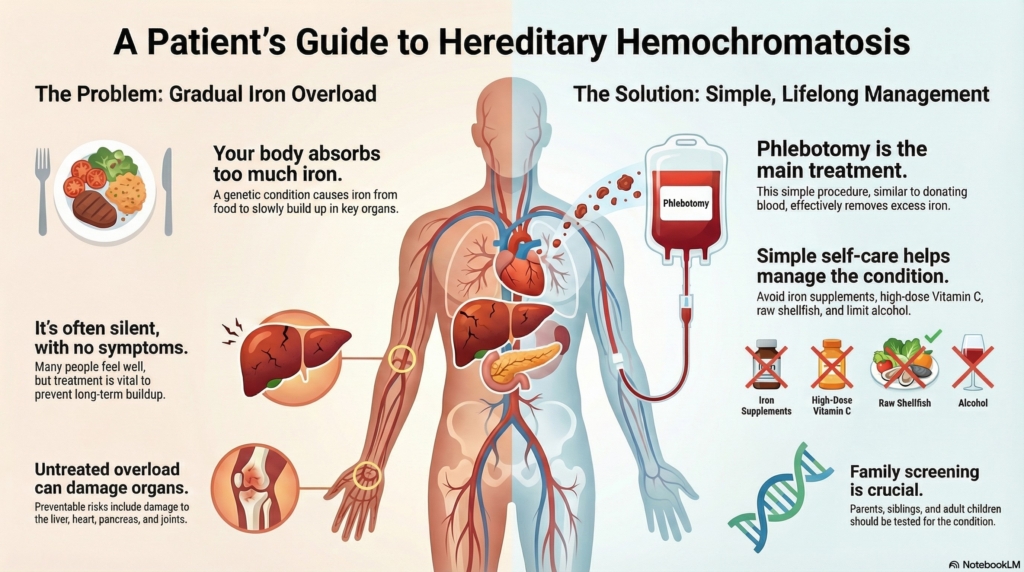
When treatment is needed, it is straightforward. Phlebotomy, which is similar to donating blood, safely removes excess iron and prevents long-term complications. With early diagnosis and routine follow-up, most people with hereditary hemochromatosis stay well and live normal, active lives.
What is hereditary hemochromatosis?
Hereditary hemochromatosis is a genetic condition in which the body absorbs too much iron from food. Extra iron gradually collects in organs such as the liver, heart, pancreas, joints, and skin.
Most cases involve the HFE gene, especially when a person inherits two C282Y variants. Other patterns, such as C282Y/H63D or H63D/H63D, usually carry much lower risk of significant iron overload. Many people with these gene changes never become ill.
Why it happens (causes)
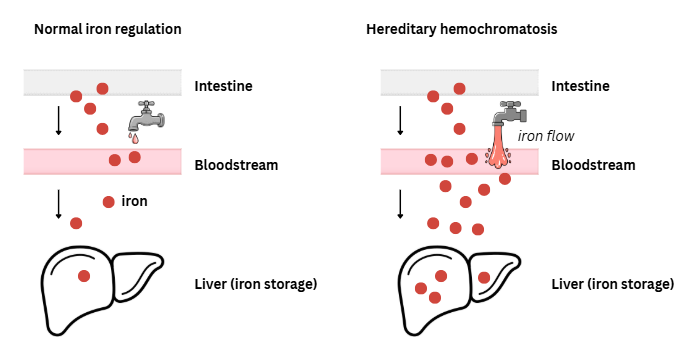
The body normally regulates iron tightly. In hereditary hemochromatosis, the “valve” that should limit absorption does not close properly, so iron continues to accumulate even when stores are already full.
Patterns include:
- C282Y/C282Y: classic type, highest likelihood of iron overload
- C282Y/H63D: usually low risk; occasional mild elevations
- H63D/H63D: rarely causes high iron
Family members may share these patterns, which is why screening first-degree relatives is recommended.
Does it cause symptoms?
Often no — many people feel completely well even when iron is elevated. Treatment is still important, because iron can silently build up over time.
When symptoms occur, they may include:
- fatigue or weakness
- joint pain, especially in the hands and wrists
- abdominal discomfort
- low libido or erectile dysfunction
- irregular periods
- bronze or gray skin color
- symptoms of diabetes
- heart rhythm changes
Without treatment, long-term iron overload can damage the liver, heart, and pancreas, which is why monitoring matters even if you feel well.
Is it dangerous?
Most people with hereditary hemochromatosis stay healthy when the condition is diagnosed and treated early.
Risk increases when:
- ferritin is very high (often >1,000 ng/mL)
- TSAT (transferrin saturation) is >45%
- liver enzymes are abnormal
- alcohol use or fatty liver disease are also present
If untreated for many years, very high iron levels can lead to cirrhosis, liver cancer, diabetes, joint disease, and heart problems—all of which are preventable with early care.
How your doctor evaluates it
Your doctor may order:
- repeat ferritin to confirm elevation
- TSAT (transferrin saturation)
- additional iron studies, when needed
- liver enzymes (ALT, AST, GGT)
- CRP/ESR to check for inflammation
- glucose and lipid profile
- HFE genetic testing (usually when TSAT >45% or there is family history)
- liver ultrasound or elastography to assess liver health
- MRI in selected cases to estimate liver iron if results are unclear
- rarely, liver biopsy when the diagnosis or stage is uncertain
Genetic testing is most meaningful when paired with persistently abnormal iron results over time.
How is it treated
The primary treatment is phlebotomy, which removes excess iron by removing blood.
Two phases:
1. Iron-reduction phase
Phlebotomy every 1–2 weeks until ferritin reaches the target range.
Target ferritin is typically 50–100 ng/mL.
2. Maintenance phase
Phlebotomy every few months to keep iron in a safe range.
Some specialists aim to keep TSAT below roughly 70%, but this is often more detail than patients need.
If phlebotomy is not possible, chelation therapy may be used.
Daily life and self-care
Most people with hereditary hemochromatosis can live fully normal lives. Your doctor may recommend:
- avoiding iron supplements
- avoiding high-dose vitamin C supplements
- limiting or avoiding alcohol, especially when ferritin or liver enzymes are high
- avoiding raw or undercooked shellfish due to infection risk
- eating a balanced diet (no need for a strict low-iron diet)
- limiting large amounts of organ meats
Many patients find phlebotomy easier than expected because it is similar to donating blood.
When should I contact my doctor?
Let your doctor know if you have:
- worsening fatigue
- new joint pain
- abdominal pain or swelling
- new skin darkening
- symptoms of diabetes
- irregular periods or erectile dysfunction
Seek urgent care if you have:
- vomiting blood
- black or bloody stools
- severe abdominal pain
- new yellowing of the skin or eyes
- chest pain, severe shortness of breath, or confusion
What is the usual plan going forward?
Your doctor will:
- monitor ferritin and TSAT periodically
- schedule phlebotomy as needed
- check liver health and metabolic markers
- recommend family screening for parents, siblings, and adult children
Family screening usually starts with iron studies, followed by genetic testing if results are abnormal or if the family mutation is known.
Most people require lifelong monitoring but feel well and remain healthy with treatment.
Making sense of it
Think of iron like water filling a slow, steady reservoir.
In hereditary hemochromatosis, the valve that normally limits iron absorption stays partly open.
Over time, the reservoir can fill too much unless some iron is periodically drained off with phlebotomy.
Hereditary hemochromatosis means your body absorbs more iron than it needs, but this usually happens gradually over many years. Seeing a mildly elevated ferritin does not mean damage is occurring right now, and many elevations are caused by factors unrelated to iron overload. The diagnosis is based on patterns over time, not a single test, and when iron levels do rise, simple treatment keeps them in a safe range. With monitoring and phlebotomy when needed, most people remain healthy and feel well.
Key takeaways
- hemochromatosis is common and treatable, and most people stay healthy with early diagnosis
- phlebotomy keeps iron levels safe, often with simple long-term monitoring
- avoid iron supplements and high-dose vitamin C, and avoid raw or undercooked shellfish
- family screening is important, especially for first-degree relatives
For clinicians: Read our detailed guide on how to communicate about HH to patients.